Mental health challenges among children and adolescents have been on the rise globally. Anxiety, depression, ADHD, and other behavioral disorders require specialized care that caters to the unique psychological and emotional needs of young individuals.
A well-designed child and adolescent mental health unit should prioritize:
Unlike adults, children and teenagers process emotions differently, making it essential to provide a therapeutic environment that fosters healing, emotional regulation, and resilience.
- Safety and Security: Minimizing risks of self-harm while allowing freedom for movement and social interaction.
- Therapeutic Spaces: Creating a calming and engaging atmosphere with dedicated areas for therapy, play, and reflection.
- Family Involvement: Encouraging parental participation in the treatment process for better outcomes.
Providing a specialized mental health facility ensures that young patients receive age-appropriate interventions in a setting that enhances their emotional well-being.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
The Child Acute Mental Health Inpatient Unit provides short term acute inpatient mental health assessment and treatment of children up to 10 to 12 years of age and adolescents up to 16 – 18 years where community approaches have proven (or are likely to prove) inadequate.
The design, layout and functionality of Child and Adolescent Mental Health Units should meet the developmental needs of their age group. Notably, the Child and Adolescent Unit should enable active family involvement in daily care, treatment and program activities including family admission and residence where appropriate.
The patients in each unit will have a broad range of mental health problems and disorders and challenging behaviours that must be managed safely and effectively.
The layout and design of the Child and Adolescent units will need to accommodate children and young people at varying stages of social, emotional and intellectual development. Young people in the Adolescent Unit will have families and others involved in their care who should feel welcome in the unit.
The unit may admit and treat patients who have:
- A risk of self injury
- A risk of self neglect
- A risk of injury to others
- A severe affective disorder
- Psychosis including early onset schizophrenia
- Pervasive developmental disorders
- Anorexia nervosa and related eating disorders
- Severe anxiety disorders
- Obsessive compulsive disorder
- Tourette’s syndrome
- Co-morbid drug and alcohol problems
- Severe family relationship difficulties.
2) Planning of child & adolescent mental health unit
i) Models of Care
Models of care include:
- Children and adolescents together in a fully integrated unit, with separate programs and activities for relevant age groups; this arrangement optimises staffing and enables efficient use of resources;
- Children and adolescents in the same unit but separate “zones” designed to cater for their differing needs; they should operate as two discrete service types with separate functional areas, programs and activities although co-location allows sharing of facilities
- Inclusion of a secured dedicated unit collocated with a paediatric precinct to allow children to participate in activities with other children such as school and play therapy
- Collocation of a Day Unit to minimise the need for hospitalisation; the Day unit would provide for day activities and close down at night.
ii) Functional Areas
The Unit will cater for both male and female patient and family members as required. The Unit should provide Bedrooms that can accommodate family members in a bed sitting arrangement with a separate bedroom to the child, with a shared Ensuite.
Support areas required in Child/ Adolescent Units will include:
- Multipurpose Group Therapy/ Activity rooms that can also be used for education purposes
- Large Interview Rooms to accommodate families
- Outdoor space for recreation activities.
- Storage for general ward equipment, occupational therapy equipment and a range of age appropriate, therapy, sport and recreation equipment in each setting.
Office accommodation should be located in a non-patient area of the unit with secured access/ egress.
Assessment / medication room (May be a shared facility)
The Unit will include a suitably equipped room for physical/ neurological examinations which will also contain locked cupboards for dressings, medications and emergency equipment in keeping with legislative requirements. The Room will require two entry/ exit doors.
External relaxation / activities areas
Each unit will require discrete and separate outdoor relaxation areas. These areas will not be locked but access to and from the units should be only from the respective unit and easily observed and monitored by staff.
Staff should however be able to prevent access to these areas at night. A common external activity area may be shared if units are co-located.
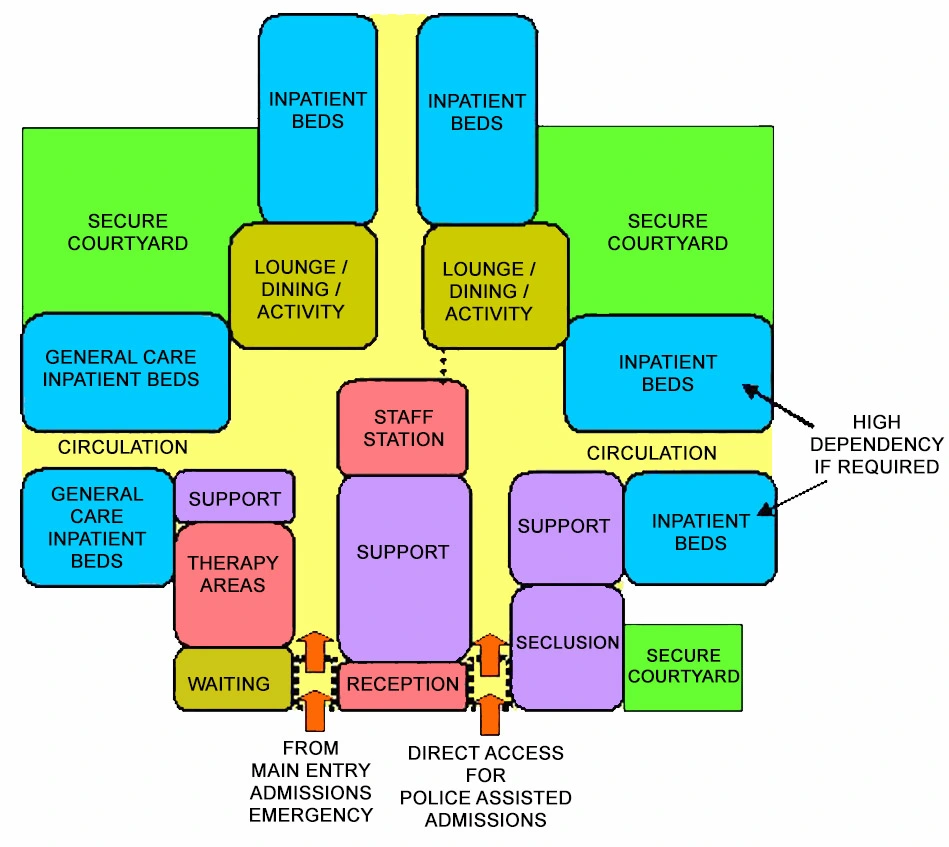
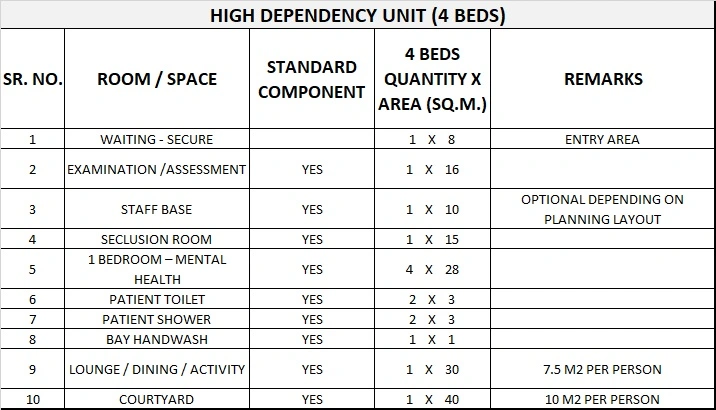
High dependency / intensive care unit (Adolescent unit only)
The Adolescent Unit will require a lockable high dependency unit consisting of at least one seclusion room and toilet/bath/ shower room opening onto a locked lounge area which has direct access to an external secure courtyard separate to other external recreation areas.
Entry to this area directly from outside the unit will be required for police assisted admissions or where a young person is highly disturbed and at immediate risk of harm to themselves or others.
Patient bedrooms
Single Patient Bedrooms shall be provided, each with an Ensuite. The patient bedroom doors must be able to be unlocked from the outside, even if locked on the inside. It is advisable to have the capacity to restrict the access to the Ensuite.
The fittings and furniture include:
- Built-in wardrobe
- Built-in desk
- Pinboard for photos and posters.
Fittings must not provide opportunities for self harm and are to have a breaking strain of less than 15 kg. Blinds to external windows are to be within double glazing. Chairs should be light weight and flexible.
Services will include the following:
- Two power outlets – RCD protected
- Staff alarm system.
- Medical gases will not be required.
Patient ensuites
An Ensuite shall be provided to each bedroom to comply with Standard Components Ensuite – Mental Health. The fittings must not provide opportunities for self harm and are to have a breaking strain of less than 15 kg.
Parent / Family / Carer bedrooms
Bedrooms for parents or other family members should include a double bed and a single bed and be of sufficient size to allow a fold away cot for very young children.
A shared Ensuite to enable parents/ carers to look after their child accommodated in another room should be available to each parent/ family/ carer bedroom.
Reception / Entry area
The entrance to each unit should be readily observable from the nursing station/office and should incorporate a greeting/ waiting area for family, friends and others which is separated from all other functional areas on the units.
The area should assist staff to prevent unauthorised entry to the unit and to provide a safe and therapeutic environment for children, adolescents and family members, (passive observation of the patient activity / recreation area from the ward office / nurses station is desirable).
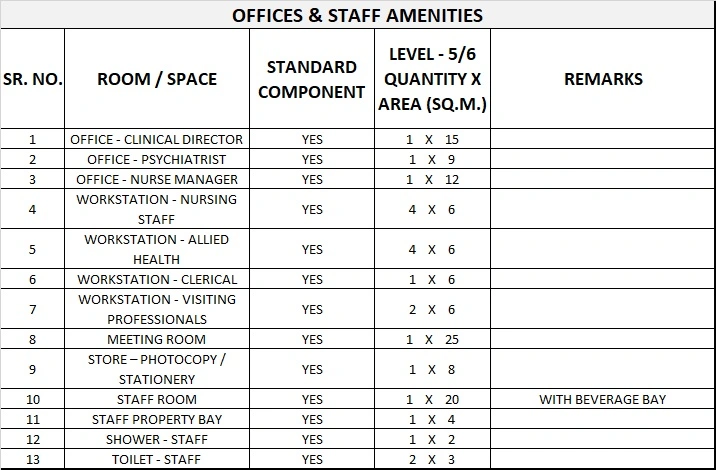
Office accommodation
Offices and workstations shall be provided according to the Operational Policy and staffing establishment. The office area should be located in the ‘patient free’ area of the unit. Administrative and office areas may be shared with adjacent units.
iii) Functional Relationships
The Child and Adolescent Acute Psychiatric Inpatient Units shall have functional relationships with the following units, services and organizations:
- Emergency Unit
- Paediatric Inpatient Unit
- Paediatric Outpatient services
- Diagnostic Pathology Unit
- Allied Health Unit
- Early childhood services
- Child and family support services
- Community services including day programs
- Drug treatment services
- Adult Psychiatric Services
- Adolescent medical units.
3) Design of child & adolescent mental health unit
i) General
The Child and Adolescent Psychiatric Unit should be located on the ground floor.
The following design issues are mandatory requirements:
- Access to the Unit must not be through other units, also the unit must not form a thoroughfare to any other unit
- Bedrooms should provide a comfortable domestic environment with comfortable, robust furniture and furnishings
- All glazing must be a grade of safety glass suitable for mental health applications
- Where co-located, the Child and Adolescent Acute Psychiatric Inpatient Units should allow full independent operation and separation while enabling common use of appropriate facilities
- Rooms and equipment need to meet the therapeutic and educational requirements of the patient group, with provisions for video conferencing in at least one large family Meeting Room and video recording in at least one Interview Room or wet and dry Therapy/ Play Room.
- The Entry areas to both Units require a Visitors’ Toilet – Disabled with baby change facilities and a Waiting Area in close proximity.
- Design elements incorporating additional security measures should not be evident to the casual observer.
ii) Environmental Considerations
Acoustics
Acoustic treatment should be applied to the following areas:
- Day Areas such as patient living, dining and activities areas
- Patient Bedrooms including high dependency, intensive care and seclusion rooms
- Consulting Rooms
- Admission Areas.
In acoustically treated rooms, return air grilles should be acoustically treated to avoid transfer of conversations to adjacent areas. Door grilles to these areas should be avoided.
Windows and Glazing
Wherever possible, the use of natural light is to be maximised. For glazing, graduate the impact resistance of the glass from toughest at lower level to weakest at high level.
In areas where damage to glass may be expected, avoid larger pane sizes. Smaller panes are inherently stronger for a given thickness than larger panes.
Where toughened glass is used it should be treated with a protective film to ensure glass is held together when broken. Laminated / toughened glass of various thicknesses should be installed dependent upon the likelihood of patient injury or building damage.
All windows and observation panels shall be glazed with a grade of safety glass suitable for mental health applications. Polycarbonate is not recommended due to surface scratching which will reduce visibility over time.
Where windows are openable, effective security features such as narrow windows that will not allow patient escape, shall be provided. Locks, under the control of staff, shall be fitted.
iii) Space Standards and Components
Provide space for key areas according to the following guide:
- Lounge/ Activities areas for social activities, 3.5 m2 per patient minimum
- Activities/ Dining areas, 5.5 m2 per patient, minimum.
- Separate Dining area 1.5m2 per patient.
- Courtyard and Terrace – minimum area – 20m2
- Outdoor areas (courtyards and terraces) – General – 5m2 per person
iv) Safety and Security
The entry to the Child and Adolescent Acute Psychiatric Inpatient Units should have a direct view of the Reception / Staff Station. Security features are required at all entrances and exits.
These may include electronic locking, intercoms, and video surveillance. A separate secured entry may be required for patients arriving with a police escort (applicable to Adolescent Units only).
All Meeting, Counselling, Group Therapy, Family Therapy and Review Board Meeting rooms require two means of egress and a duress alarm.
v) Fixtures and Fittings
Furniture should be robust but light weight and designed to minimise damage or injury if thrown. Fixtures and fittings should be safe and durable and avoid the potential to be used either as a weapon or to inflict personal damage.
Generally, all fixings should be heavy duty, concealed, and where exposed, tamper proof. Fittings, including hooks, curtain tracks, bathroom fittings, should be plastic where possible, and have a breaking strain of not more than 15kgs.
Paintings, mirrors and signage should be rigidly fixed to walls with tamper proof fixings. Mirrors shall be of safety glass or other appropriate impact resistant and shatterproof construction. They shall be fully glued to a backing to prevent availability of loose fragments of broken glass.
Holland blinds, Venetian blinds and curtains should be avoided in patient areas. Curtain tracks, pelmets and other fittings that provide potential for patients to hang themselves should be avoided or designed so that the potential is removed.
vi) Building Services Requirements
Avoid exposed services; for example, sink wastes which may be easily damaged.
4) Components of the Unit
The Child and Adolescent Acute Psychiatric Inpatient Unit will consist of a combination of Standard Components and Non-Standard Components.
Provide the Standard Components to comply with details in Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets.
i) Non-Standard Components
Play therapy room
Description and Function – A Play Therapy Room shall be provided for ‘regressive’ therapies such as artwork, doll play and clay modelling. The room shall be designed with the young child 10-12 years in mind.
Location and Relationships – The Play Therapy Room should be located within the patient treatment / therapy zone of the Unit.
Considerations – Fittings, fixtures and equipment will include:
- Bench, open under
- Storage cupboards for materials
- Whiteboard
- Chairs
- Hand basin with soap and paper towel fittings.
Finishes should be smooth and easily cleaned, flooring should be vinyl.
Recreation / Day area
Description and Function – A Recreation / Day area shall be provided for a wide range of activities including watching TV, listening to music, computer and other activities.
Location and Relationships – The area requires ready access to the secured courtyard and must be overseen from the Staff Station.
Considerations – Fittings and furniture should be suitable for children up to 10-12 years, for teenagers up to the age of 18 and visiting family members.
Quiet / Time out room
Description and Function – The unit will require a room to be used for quiet time/ time out for agitated and distressed children. The room will be lockable and permit observation by staff while providing privacy to the room occupant.
Location and Relationships – The room should be located in an area that will minimise disruption to unit activities. The room should have ready access to a toilet and washing facilities close by that does not require traversing the unit.
Considerations – The room will be very plain and simple with unbreakable fittings. The room will be similar to Lounge- Patient, suitable for mental health areas. Television, DVD and CD players are not permitted in this room,
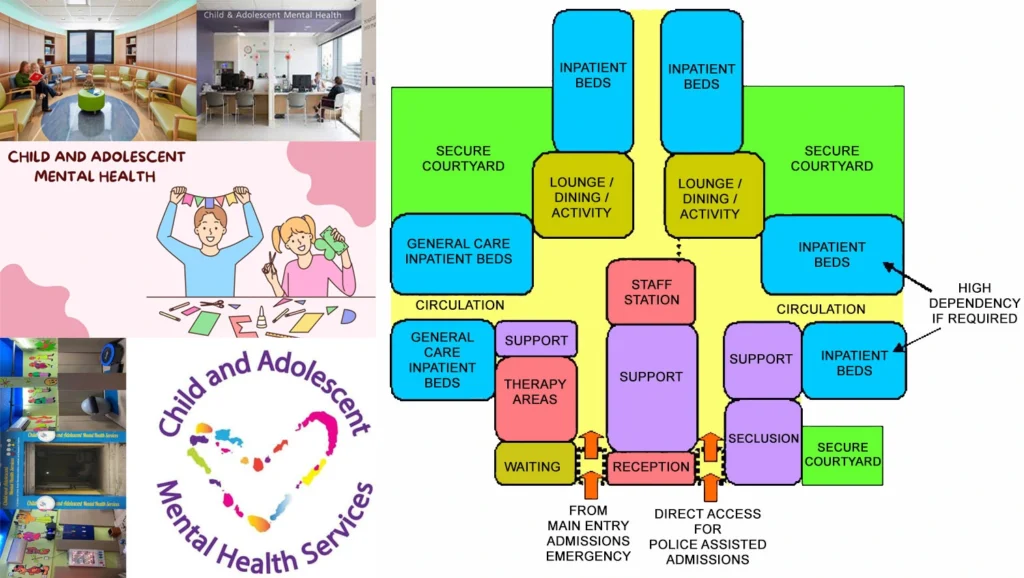
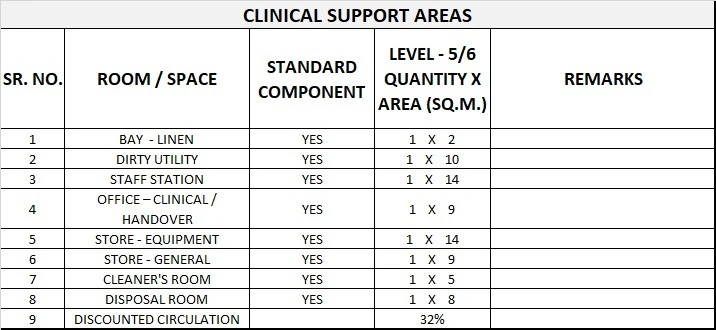
5) Schedule of Accommodation
Child & Adolescent Mental Health Unit Generic Schedule of Accommodation
Schedule of Accommodation for a Child & Adolescent Acute Mental Health for Levels 5/6
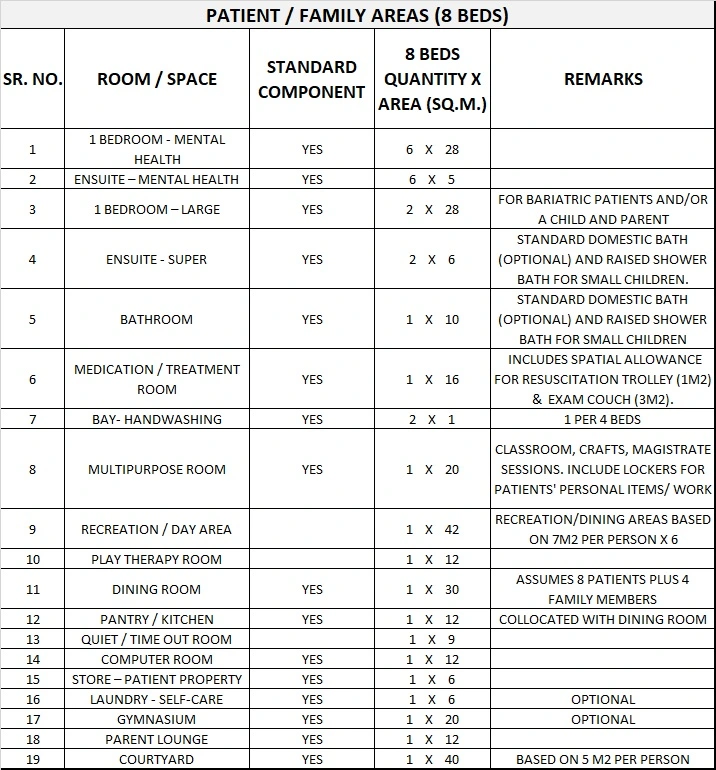
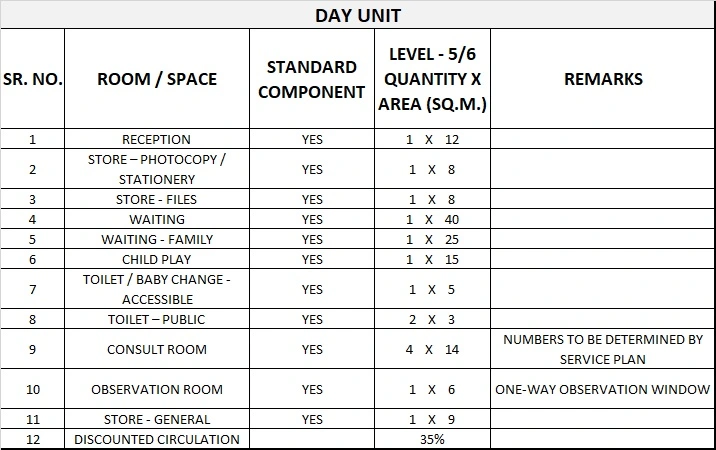
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
6) Functional Relationship Diagram
Child & Adolescent Mental Health Unit Functional Relationship Diagram