Community Health Units (CHUs) serve as the foundation of primary healthcare delivery, especially in underserved and rural areas. These units provide essential medical services, including preventive care, maternal and child health, immunizations, and treatment for common illnesses.
CHUs act as the first point of contact between communities and healthcare systems, ensuring affordable, accessible, and continuous healthcare services.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
This Guideline is a resource to assist with the planning, design and construction of a Community Health Centre (CHC). It must be read in conjunction with generic requirements and Standard Components, which are described in other parts of these Guidelines.
Community Health Centres may also contain facilities that are more fully covered by other unit specific Guidelines e.g. Outpatients Unit and Rehabilitation.
i) Description
Community Health facilities can range from single rooms to multi-functional clinics and can either be integrated within a Hospital Facility or could be a stand-alone building. Specific requirements for the Facility are determined by the range of services to be provided.
ii) Function
The primary role of a Community Health Centre is to facilitate the delivery of health care services to clients, whilst also providing suitable facilities to meet the working needs of staff.
Activities undertaken include counselling, therapy, health education, community support and group programmes. Community Health Services are typically delivered in a community based rather than hospital based setting.
A Community Health Centre may be the physical base for a service rather than where the service is delivered or a combination of both.
Some Community Health Services could also be provided in an Outpatients facility. This will be dictated by the Services plan for the facility.
iii) Services Provided
Services that may be included in a Community Health Centre include:
Primary Health Care
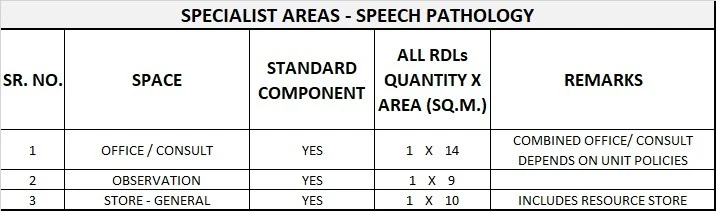
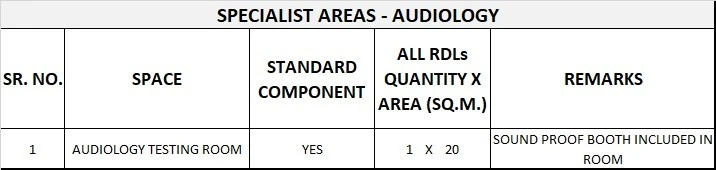
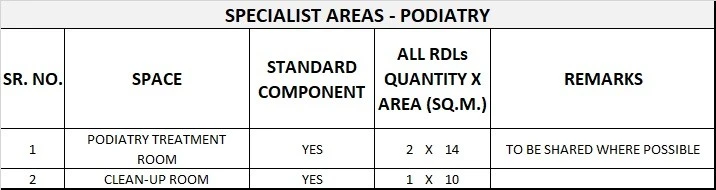
- Allied Health services including Physiotherapy; Occupational Therapy; Podiatry; Chiropractic; Social work; Speech pathology; Psychology; Audiology; Health Education (eg Asthma, Diabetes); Multicultural health services; Primary medical services (GPs and nurse practitioners);
- Outpatients and post-acute care services;
- Antenatal / Postnatal clinics;
- Aged Care services
- Chronic disease management services;
- Continence services;
- Counselling services (eg Bereavement, Adolescents, Problem Gambling, Generalist);
- Child assessment, early childhood services, youth and family health services;
- Child Protection Services (including developmental issues, early intervention services and child protection counselling);
- Dietetics & Nutrition
- Dental services;
- Family planning;
- HIV/AIDS services;
- Home nursing services & Outreach Medical Clinics;
- Men’s health services;
- Palliative care and Rehabilitation services
- Sexual Health & Sexual Assault services;
- Women’s health services.
2) Planning of Community health unit
i) Operational Models
Hours of Operation
The Community Health Unit will generally operate up to 12 hours per day, 5 days per week with some specific services available 24 Hours a day.
There is an increasing trend towards ‘extended hours’ services. Outreach services (eg community nursing) may be provided over weekends and public holidays. Out of hours access may be required on a planned basis for community groups, voluntary organisations or other specific activities.
Flexibility
As the demand for services vary over time within a Community Health Unit, a flexible accommodation model is recommended. Opportunities for sharing resources and facilities within the unit should also be examined. e.g. Reception and Waiting Areas, Interview and Treatment Rooms.
If shared spaces are maximised, it reduces the need for potentially underutilised special purpose rooms. Similarly, Operational policies should also consider sharing equipment.
Location of equipment within the unit is important and easy access to equipment for specific purposes is highly recommended. The design of the unit should ensure that there are ample opportunities for expansion and adaptation for future use.
ii) Operational Policies
Operational policies should be clearly articulated as it can have major impact on facility management and the capital and recurrent costs of health facilities.
Operational policies may vary depending on various factors and it is recommended that users of the unit define their own operational policies.
Staffing Levels
Staffing levels will vary for each CHC, depending on Operational Policies, services provided, availability of staff, case mix and activity levels.
iii) Planning Models
Location – The location of CHCs will vary, depending on the outcome of Service Planning at an Area Health Service level. Options for locating centres include:
- free standing in a community location;
- attached or included in the development of commercial facilities e.g. shopping centres;
- On the grounds of a hospital facility.
Configuration – The configuration of a CHC will depend on:
- Population profile
- Service mix
- Staff profile providing the services
- Relationship of the CHC with adjacent hospital facility
iv) Functional Areas
Functional Zones
Individual spaces combine to form zones or groups of spaces with a similar purpose. The relationship between zones is considered important to ensure that CHCs operate efficiently and effectively.
A Community Health Centre can be subdivided into three key Functional Zones:
- Main Entry / Reception;
- Client Areas – activities and treatment including specialist areas such as Occupational Therapy, Physiotherapy, Cardiac, Dental facilities etc.
- Staff Areas.
Client Areas / Specialist Areas
Specialist clinical areas such as Occupational Therapy, Physiotherapy, Prosthetist, Orthotist, may be sited in close proximity to each other so that where possible they can share facilities such as outdoor treatment areas and splinting activities.
Physiotherapy and Occupational Therapy staff should have visibility to the treatment areas from their offices. Direct access to an outdoor area from the clinical area is required for Occupational Therapy and Physiotherapy.
Occupational Therapy requires a relatively large treatment area to facilitate individual function activities, activities of daily living, evaluation of equipment needs and group therapeutic activities.
If Physiotherapy is to be provided, an area is required to facilitate evaluation, therapeutic exercise and ambulation training. The treatment area needs to accommodate equipment such as electrotherapy machines, several plinths, gym equipment, mats, treatment tables, parallel bars and steps.
A specifically designated area should be provided where electric treatment modalities are required for Physiotherapy. A suitable variety and number of counselling/interview rooms should be provided for use by psychologists, social workers and counsellors.
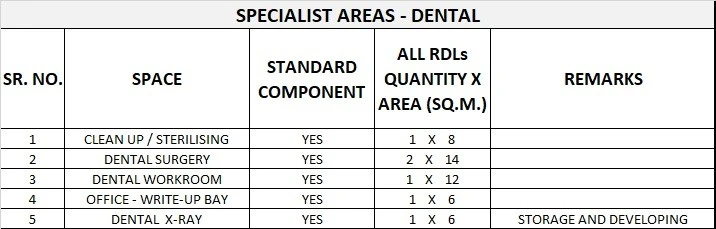
Dental Facilities
Depending on the CHC, there may be a specifically designated Dentistry Consulting Room or a sessional dentist and dental nurse may share accommodation with a Podiatrist.
If Dental facilities are included, there will be a need for space for sterilising equipment, portable X-Ray and X-Ray developing equipment.
Design of the area for decontamination and sterilising must comply with the relevant Australian Standard. Areas for Dentistry or Podiatry need to be investigated to allow room for specialised equipment including chairs.
The Dental Facilities should be located with ready access to the Main Entry and Waiting Areas. The Dental facilities must be acoustically isolated and it may be better to separate them from other areas.
Please refer “Acoustic Solutions for Healthcare Facilities”. Access is required for patients using mobility aids such as walking frames or wheelchairs.
v) Functional Relationships
Where possible, Community Health Centres should be in a quiet location, with a pleasant outlook and maximum environmental benefits. A CHC should be located in an area that is accessible to the community by both public and private transport and in close proximity to other local resources.
Ideally this location will adjoin other public amenities routinely used by the community e.g. shopping precinct, transport hub, library. It should be noted that a CHC services may be located over more than one site and in more than one community.
Access
Off-street access for vehicles transporting clients must be provided. Easy access is required to Car Parking Areas and other Health Care Facilities on the site if provided.
Some services may require a separate and discreet entry point. Ambulance access must be provided to the facility with trolley access to the Main Entry, Waiting and all Client Areas.
All-weather vehicle drop-off points should be provided for easy access by clients who are elderly, frail, have limited mobility or who are wheelchair bound.
Internal
The internal plan of the CHC must allow clients to easily move to and from treatment and activity areas, and enable efficient staffing.
Optimum internal relationships include:
- Reception / Clerical Areas should have a clear view of Main Entry / Waiting Areas and be visible from adjacent Staff Areas. There should be easy access to stationery and medical records. The Reception Area should provide a barrier controlling access between Waiting and Treatment Areas.
- Consultation / Examination / Interview Rooms should be easily accessible from the Main Entry / Waiting Area as well as the Staff Area;
- Meeting / Activity Rooms should be adjacent to the Main Entry / Waiting Area so they can be accessed after hours, with the rest of the centre safely secure.
- Staff areas must be designed so they allow staff to easily move between the Main Entry / Reception and Client Areas. Staff offices and amenities should be separate from Client and Public Areas to provide privacy and a quiet work area.
3) Design of Community health unit
1) Parking
Generally car parking will be provided for clients and staff. In particular, times of attendance for staff and overnight parking for health service vehicles will impact on requirements.
Security issues need to be addressed when planning for after-hours parking. These issues will vary from site to site, and will need to be determined in accordance with Local Authority requirements.
ii) Disaster Management
The potential role of Community Health Centres in a disaster management situation should be assessed.
Attributes which make it potentially useful in a disaster situation include:
- large open spaces for disaster management or emergency accommodation;
- Consult / Interview Rooms for assessment of victims;
- Focal point in the community.
iii) Infection Control
Consideration of Infection Control is important in the design of this Unit. Treatment spaces will be used for a variety of clients. It is possible that infectious patients will use the same treatment spaces as immuno-suppressed patients at different times on the same day.
Standard precautions must be taken for all clients regardless of their diagnosis or presumed infectious status. Refer to Guidelines for further information. Staff hand washing facilities, including disposable paper towels, must be readily available.
iv) Environmental Considerations
Acoustics
The CHC will require consideration of acoustic privacy including:
- Interviews with clients;
- Location noisy areas such as Public Waiting, Dental, Child Health Facilities;
- Meeting rooms for staff discussion
- Exclusion of distracting noises during client consultations
Solutions to be considered should include sound absorbing materials and sound isolating construction, separation of quiet areas from noisy areas etc. Please refer to “Acoustic Solutions for Healthcare Facilities”
Natural Light
Natural lighting is important for the wellbeing of patient and staff and assists in orientation of building users which leads to improved service outcomes.
The use of natural light should be maximised throughout the Unit. Access to natural light is desirable and highly recommended.
Privacy
For the purpose of Patient privacy and confidentiality, it is important to consider the following:
- Confidentiality of client discussions and records;
- Provision of sub-waiting areas for clients wishing or needing to be separated;
- Location of windows and doors to ensure privacy of clients.
v) Safety and Security
The facility should provide a safe and secure environment for patients, staff and visitors while remaining a non-threatening and supportive atmosphere conducive to the delivery of services.
The facility should cater to patients with varying levels of physical and mental capabilities. The facility, furniture, fittings and equipment must be designed and constructed so as to minimise risks of injury.
Adequate security should be provided to prevent violence and theft in Health Care Facilities. Internal spaces and zones should offer a high standard of security through grouping functions, controlling access and egress from the Unit and providing optimum observation for staff.
The level of observation and visibility has security implications. Planning should allow for after hours access to Public Areas without compromising security of Staff Areas.
vi) Finishes
Interior Design
The design of internal spaces with respect to furnishings, style, colour, textures, ambience, perception etc can assist in relaxing patients and preventing an institutional atmosphere.
However, cleaning, infection control, fire safety, client service and the patient’s perception of a professional environment must always be considered.
Some interior spaces may have restrictions on colour due to the nature of its function such as clinical observation in treatment areas. Bold primary colours should be avoided in such areas
vii) Building Services Requirements
Unit design should address the following Information Technology / Communications issues:
- Paperless records;
- Handheld computers, email & Paging and personal telephones replacing some aspects of call systems;
- Picture Archiving Communication System (PACS);
- Data entry including scripts and investigation requests;
- Bar coding of supplies and X-Rays / records.
- Data and communication outlets at regular intervals to enable electronic use of records.
Nurse call & Alarm systems
The need for provision of a call system that allows clients and staff to alert other health care staff in a discreet manner at all times should be considered.
A discreet duress alarm system will be required at all Reception Points and Client Treatment Areas, where a staff member may be alone with a client.
4) Components of the Unit
The Community Health Centre will contain a combination of Standard Components and Non-Standard Components. Provide Standard Components to comply with details in the Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets.
i) Non Standard Components
Provide the Non Standard Components as described in this section, according to Operational Policy and service demand.
Entry Canopy
Description and Function – An Entry Canopy is required to provide undercover access to the building from vehicles. Depending on the type of transportation vehicles expected at the facility, the canopy should be large enough to allow manoeuvring beneath it.
Location and Relationships – Provide at Main Entry.
Main Entry
Description and Function – The Main Entry to the facility should be clearly displayed through appropriate signage informing people where to proceed. The Entry may incorporate an airlock space and should have proper weather protection. Entry doors should cater to the physically handicapped and may require automatic doors for easy access.
Location and Relationships – This should be located adjacent to a vehicle set down point and readily accessible from the street and parking areas. Reception and Waiting Areas should be adjacent.
Treatment Cubicle – Physiotherapy / Occupational Therapy
Description and Function – Treatment cubicles provided for Physiotherapy and Occupational Therapy will comply with Standard Component Patient Bay – Non-Acute Treatment. Bays may be provided as enclosed rooms for additional privacy.
Location and Relationships – Treatment bays and rooms will require close access to waiting areas for patient access and plaster rooms and other treatment spaces for staff access.
Considerations – In addition to the provisions noted in Standard Components the following may be included:
- Plinth, adjustable height, some may be double size
- Mesh and pulleys for exercises to sides and ceiling space over the plinth
5) Schedule of Accommodation
i) Community Health Generic Schedule of Accommodation
The content and size of a Community Health Centre varies depending on the location, services provided and throughput. Community Health Services are categorised into six levels of service. However, these do not necessarily lead to
different physical requirements.
A generic Schedule of Accommodation follows that lists generic spaces that can be combined to form a Community Health Centre. Sizes and quantity of each space will need to be determined on a case by case basis.
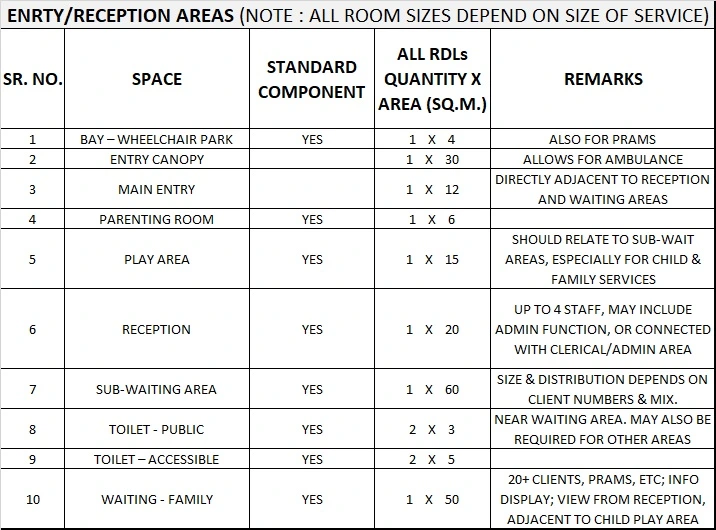
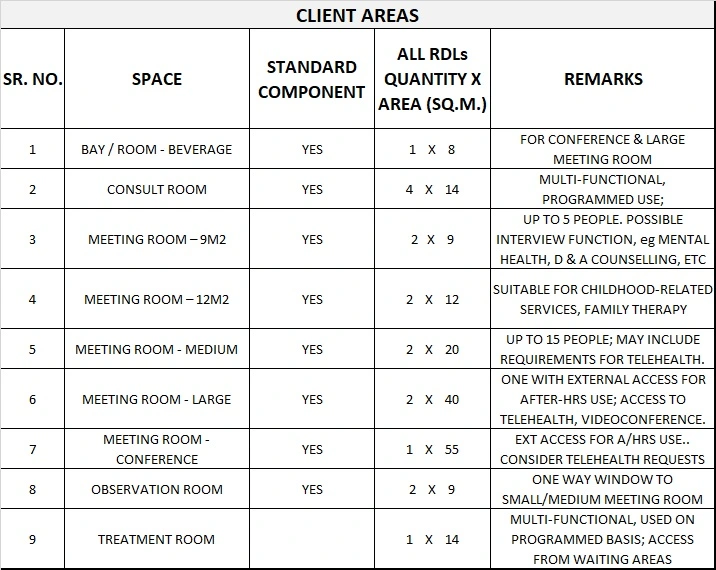




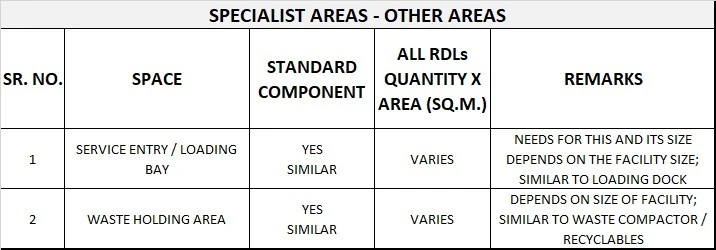
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of
- individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
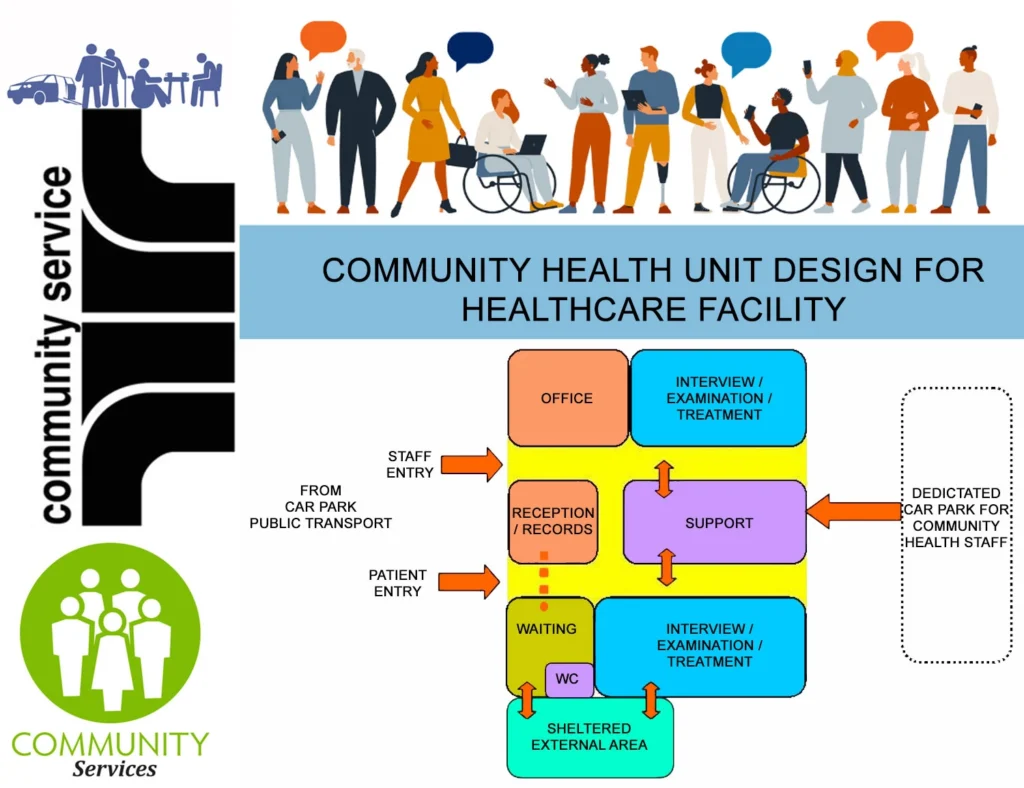
6) Functional Relationship Diagram
Community Health Functional Relationship Diagram




Very nice .We are interested