India’s healthcare delivery system is structured as a three-tier system designed to ensure equitable access to health services for every citizen, especially those in rural and underserved areas.
The tiers include Sub-Centres (SCs), Primary Health Centres (PHCs), and Community Health Centres (CHCs)—each playing a crucial role in public health infrastructure.
Among these, Sub-Centres are the first point of contact between the healthcare system and the community. Strategically located in rural areas, they serve populations of 3,000 to 5,000 people and act as the frontline units for delivering essential health services like maternal and child healthcare, immunizations, family planning, sanitation, and disease prevention.
To standardize and enhance the quality of services across these facilities, the Government of India introduced the Indian Public Health Standards (IPHS) under the National Rural Health Mission (NRHM) in 2005.
The IPHS framework provides clear guidelines for infrastructure, human resources, equipment, service delivery, and performance monitoring. These standards aim to improve accountability, accessibility, and reliability of public healthcare facilities—starting from the sub-centre level and scaling upward.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
In the public sector, a Health Sub-centre is the most peripheral and first point of contact between the primary health care system and the community.
A Sub-centre provides interface with the community at the grass-root level, providing all the primary health care services. It is the lowest rung of a referral pyramid of health facilities consisting of the Sub-centres, Primary Health Centers, Community Health Centres, Sub-Divisional/Sub-District Hospitals and District Hospitals.
The purpose of the Health Sub centre is largely preventive and promotive, but it also provides a basic level of curative care.
As per population norms, there shall be one Sub-centre established for every 5000 population in plain areas and for every 3000 population in hilly/tribal/desert areas.
As the population density in the country is not uniform, application of same norm all over the country is not advisable. The number of Sub-centres and number of ANMs shall also depend upon the case load of the facility and distance of the village/habitations which comprise the Sub-centres.
There are 147069 Sub-centers functioning in the country as on March 2010 as per Rural Health Statistics bulletin, 2010.
The Indian Public Health Standards (IPHS) for health Sub-centre lays down the package of services that the Sub-centre shall provide the population norms for which it would be established, the human resource, infrastructure, equipment and supplies that would be needed to deliver these services with quality.
Setting standards is a dynamic process. These standards are being prescribed in the context of current health priorities and available resources. The Indian Public Health Standards (IPHS) are being prescribed to provide basic primary health care services to the community and achieve and maintain an acceptable standard of quality of care.
During the course of revision of current IPHS for Sub- centre, feedback through interactions with Health Worker Females/Auxillary Nurse and Mid-wife (ANMs) was taken regarding the wide spectrum of services that they are expected to provide, which revealed that most of the essential services enumerated are already being delivered by the Sub-centres staff.
However, the outcomes of health indicators do not match with services that are said to be provided. Therefore it is desirable that manpower as envisaged under IPHS should be provided to ensure delivery of full range of services. Monitoring of services may be strengthened for better outcomes.
2) Categorization of Sub-Centres
In view of the current highly variable situation of Sub- centres in different parts of the country and even with in the same State, they have been categorized into two types Type A and Type B.
Categorization has taken into consideration various factors namely catchment area, health seeking behavior, case load, location of other facilities like PHC / CHC / FRu / Hospitals in the vicinity of the Sub-centre.
States shall be required to categorize their Sub-centres into two types as per the guidelines given below and provide services and infrastructure accordingly. this shall result in optimum use of available resources.
Type A
type A Sub Centre will provide all recommended services except that the facilities for conducting delivery will not be available here. However, the ANMs have been trained in midwifery, they may conduct normal delivery in case of need.
If the requirement for this goes up, the sub centre may be considered for up gradation to Type B. the Sub-centres in the following situations may be included in this category.
Point – i
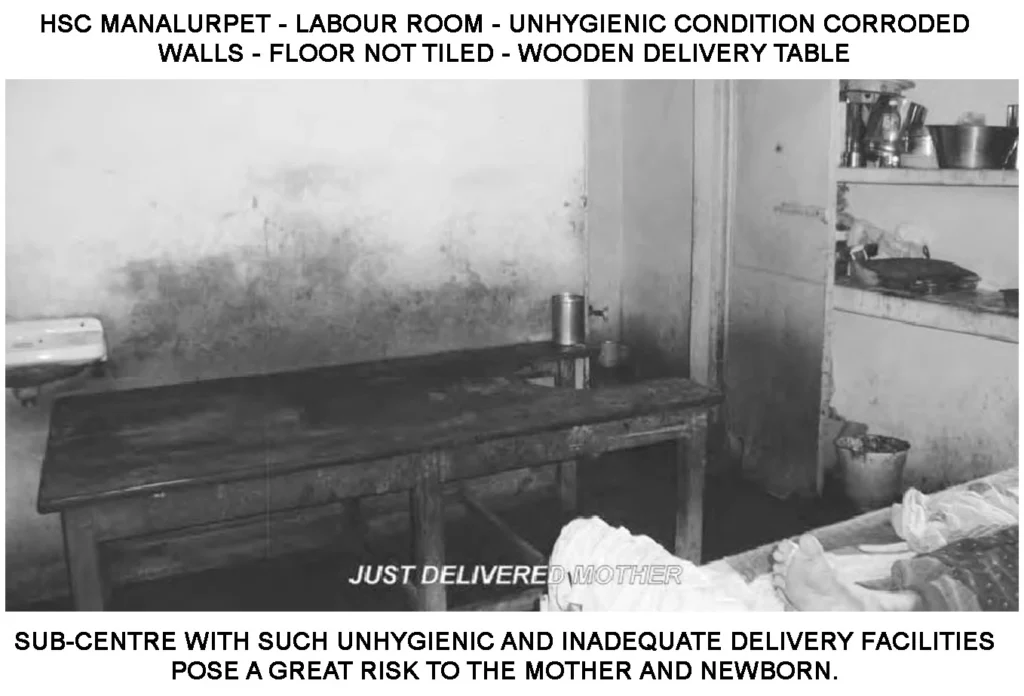
Sub-centres not having adequate space and physical infrastructure for conducting deliveries, due to which providing labour room facilities and equipment at these Sub-centres is not possible.
However there may still be demand for delivery services from the community in these areas e,g, Sub-centres located in remote, difficult, hilly, desert or tribal area.
In such areas, the transport facility is likely to be poor and the population is still dependent on these Sub-centres for availing delivery facilities.
In such situations, ANMs would be required to conduct deliveries at homes and ANMs of these Sub-centres should mandatorily be Skilled birth Attendance (SbA) trained. Such Sub-centres should be identified for infrastructure up gradation for conversion to type b Sub-centres on priority.
Point – ii
Sub-centres situated in the vicinity of other higher health facilities like PHC/CHC/FRu/Hospital, where delivery facilities are available
Point – iii
Sub-centres in headquarter area
Point – iv
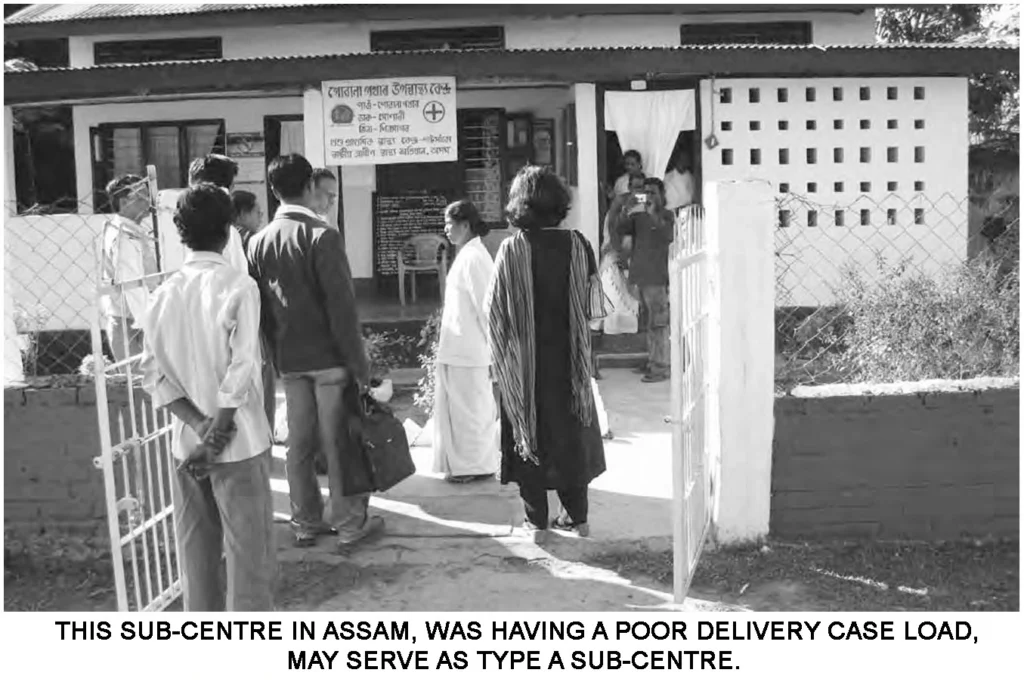
Sub-centres where at present no delivery or occasional delivery may be taking place i.e. very low case load of deliveries. If the case load increases, these Sub-centres should be considered for up gradation to Type B.
Staff recommended
One ANM (Essential), two ANMs: (Desirable to split the population between them and one of them provides outreach services and the other is available at the Sub-centre)
One Health Worker (Male) (Essential)
Sanitation services should be provided through outsourcing on part time basis
Guidelines
- The facilities for conducting delivery will not be available at these sub-centres and patients may usually be referred to nearby centers providing delivery facilities. If the requirement for delivery services goes up , the sub centre may be considered for up gradation to Type B.
- These Sub-centres should provide all other recommended services and focus on outreach services, prevalent diseases, tuberculosis, leprosy, Non-communicable diseases, nutrition, water, sanitation and epidemics. It is also to be ensured that the Staff of these sub-centres is provided training in all new programmes on priority basis and refresher training is provided regularly.
- Extra payment should be provided to Staff posted in difficult areas.
- If there is shortage, Health Worker male should be posted on priority basis in areas endemic for vector borne diseases.
Type B (MCH Sub-Centre)
This would include following types of Sub-centres:
Point – i
Centrally or better located Sub-centres with good connectivity to catchment areas.
Point – ii
They have good physical infrastructure preferably with own buildings, adequate space, residential accommodation and labour room facilities.
Point – iii
They already have good case load of deliveries from the catchment areas.
Point – iv
There are no nearby higher level delivery facilities.
Guidelines
Such Sub-centers should be developed as a delivery facility and should also cater to adjacent Type A sub- centres areas for delivery purpose. Type B Sub-centre, will provide all recommended services including facilities for conducting deliveries at the Sub-centre itself.
They will be expected to conduct around 20 deliveries in a month. they should be provided with all labour room facilities and equipment including Newborn care corner.
ANMs of these Sub-centres should be SbA trained. These centers may be provided extra equipment, drugs, supplies, materials, 2 beds and budget for smooth functioning. If number of deliveries is 20 or more in a month, then additional 2 beds will be provided.
Staff recommended
two ANM (Essential)
One Health Worker (Male) : (Essential)
One Staff Nurse or ANM (if Staff Nurse not available)
(Desirable, if number of deliveries at the Sub-centre is 20 or more in a month)
Sanitation services should be provided through outsourcing on full time basis
3) Services to be provided in a Sub-Centre
Sub-centres are expected to provide promotive, preventive and few curative primary health care services. keeping in view the changing epidemiological situation in the country, both types of Sub centres should lay emphasis on Non-Communicable Diseases related services.
Given the understanding of the health Sub-centre as mainly providing outreach facilities, where most services are not delivered in the Sub-centre building itself, the site of service delivery may be at following places:
- In the village: Village Health and Nutrition Day/ Immunization session.
- During house visits.
- During house to house surveys.
- During meetings and events with the community.
At the facility premises. It is desirable, that the Sub-centre should provide minimum of six of hours of routine OPD services in a day for six days in a week.
Wherever two ANMs are provided, it shall be ensured that one of the ANMs is available at the Sub-centre and the Sub centre remains open for providing OPD services on all working days. Only one of them may provide outreach services at a time.
The main differences in services to be provided by the two types of Sub-centres are:
Type A: Shall provide all services as envisaged for the Sub-centre except the facilities for conducting delivery will not be available here.
Type B: they will provide all recommended services including facilities for conducting deliveries at the Sub-centre itself. This Sub-centre will act as Maternal and Child Health (MCH) centre with basic facilities for conducting deliveries and Newborn Care at the Sub- centre.
Although the main focus shall be to promote institutional deliveries, however, the facilities for attending to home deliveries shall remain available at both types of Sub- centres.
The following is the consolidated list of services to be provided through two types of Sub-centres. The services have been classified as Essential (Minimum Assured Services) or Desirable (that all States/UTs should aspire to achieve).
4) Physical Infrastructure
A Sub-centre should have its own building. If that is not possible immediately, the premises with adequate space should be rented in a central location with easy access to population.
The States should also explore options of getting funds for space from other Health Programmes and other funding sources.
Location of the Centre
For all new upcoming Sub-centres, following may be ensured:
- Sub-centre to be located within the village for providing easy access to the people and safety of the ANM.
- As far as possible no person has to travel more than 3 km to reach the Sub-centre.
- While finalizing the location of the Sub-centre, the concerned Panchayat should also be consulted.
Building and Lay out
- Boundary wall/fencing: boundary wall/fencing with Gate should be provided for safety and security.
- In the typical layout of the Sub-centre, the residential facility for ANM is included, however, it may happen that some of the existing Sub-centres may not have residential facilities for ANM. In that case, some house should be available on rent in the Sub-centre headquarter village for accommodating the ANM.
- Residential facility for Health Worker (Male), if need is felt, may be provided by expanding the Sub-centre building to the first floor. the entrance to the Sub-centre should be well lit and easy to locate. It should have provision for easy access for disabled and elderly. Provision of ramp with railing to be made for use of wheel chair/stretcher trolley, wherever feasible.
- The minimum covered area of a Sub-centre along with residential quarter for ANM will vary depending on land availability, type of Sub-centre and resources.
- Separate entrance for the Sub-centre and for the ANM quarter may be ensured
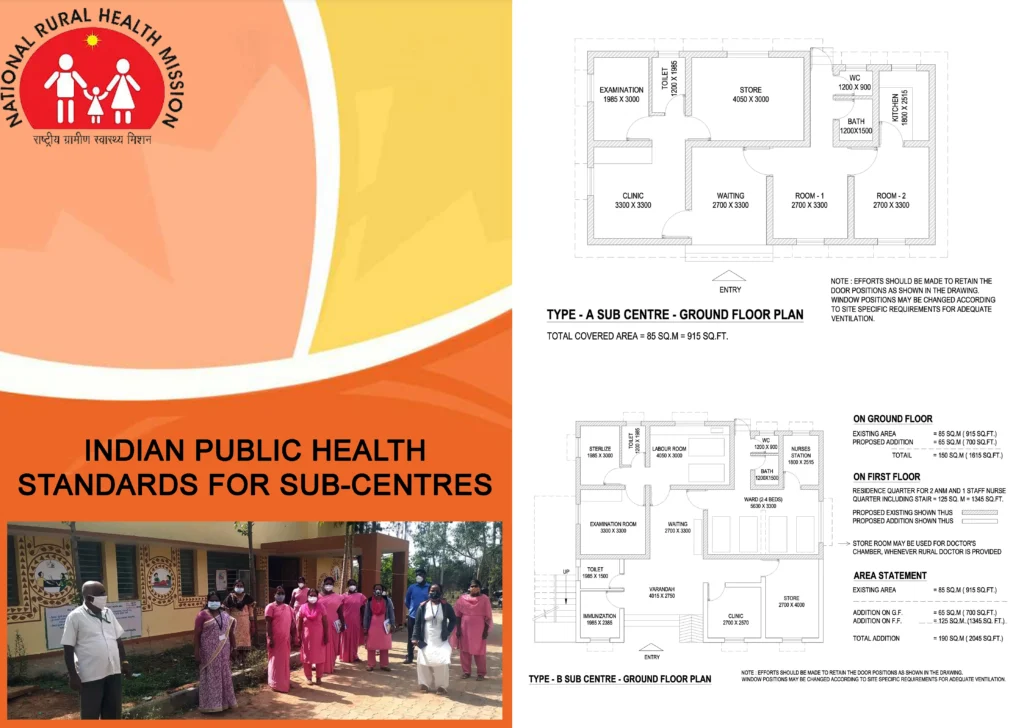
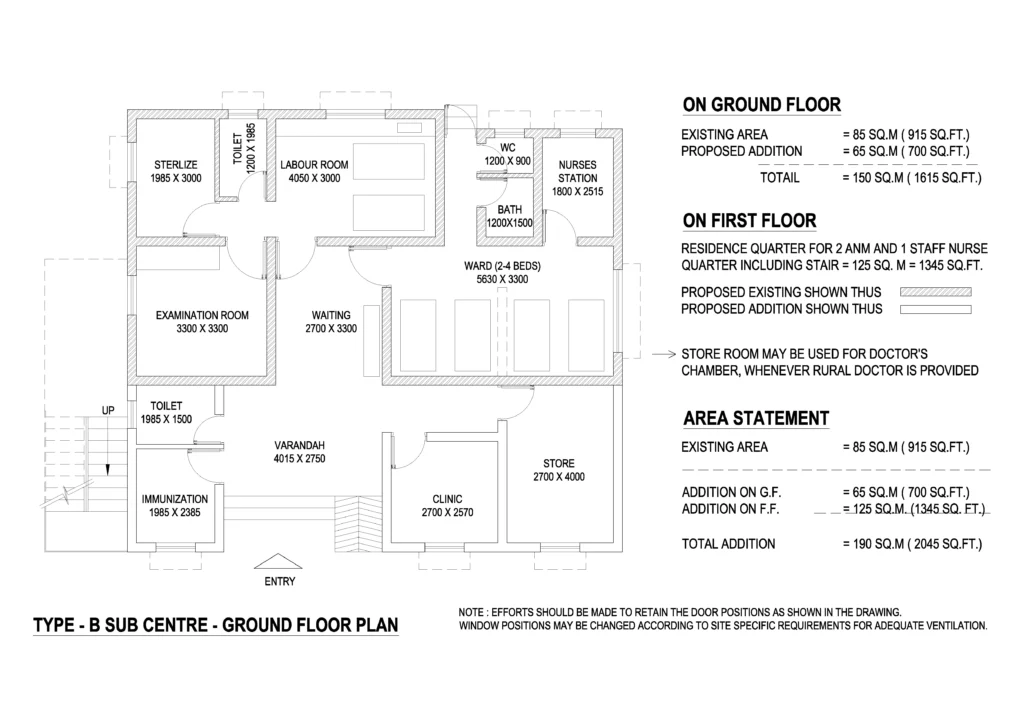
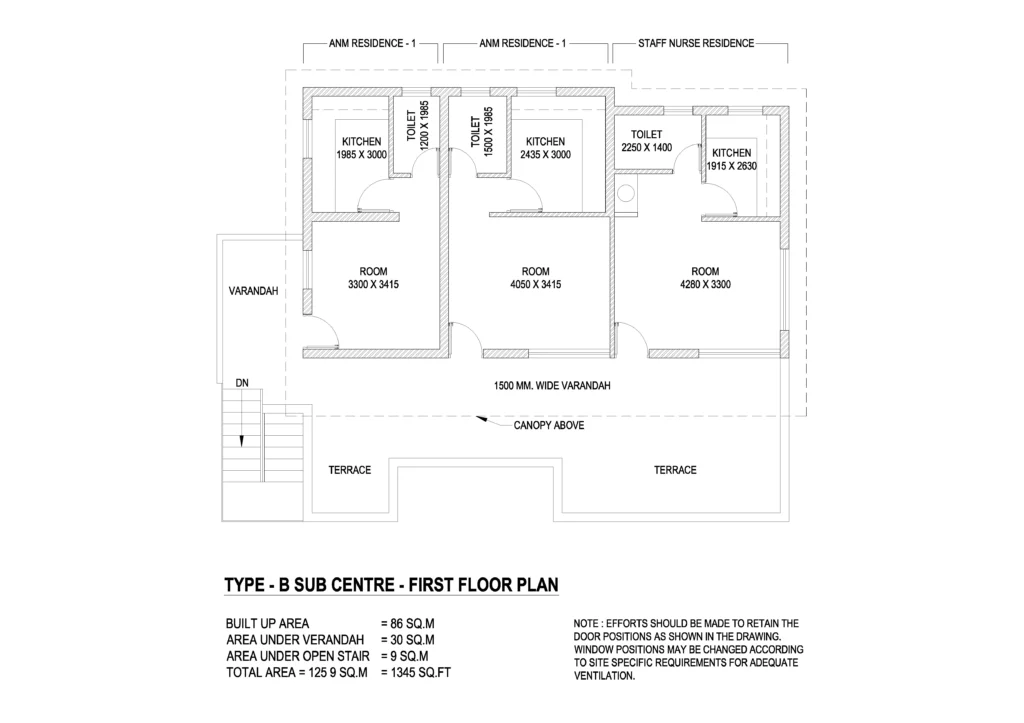
Type B Sub-centre should have, about 4 to 5 rooms with facilities of
- Waiting Room
- One Labour Room with one labour table and Newborn corner
- One room with two to four beds (in case the no. of deliveries at the Sub-centre is 20 or more, four beds will be provided)
- One room for store
- One room for clinic/office
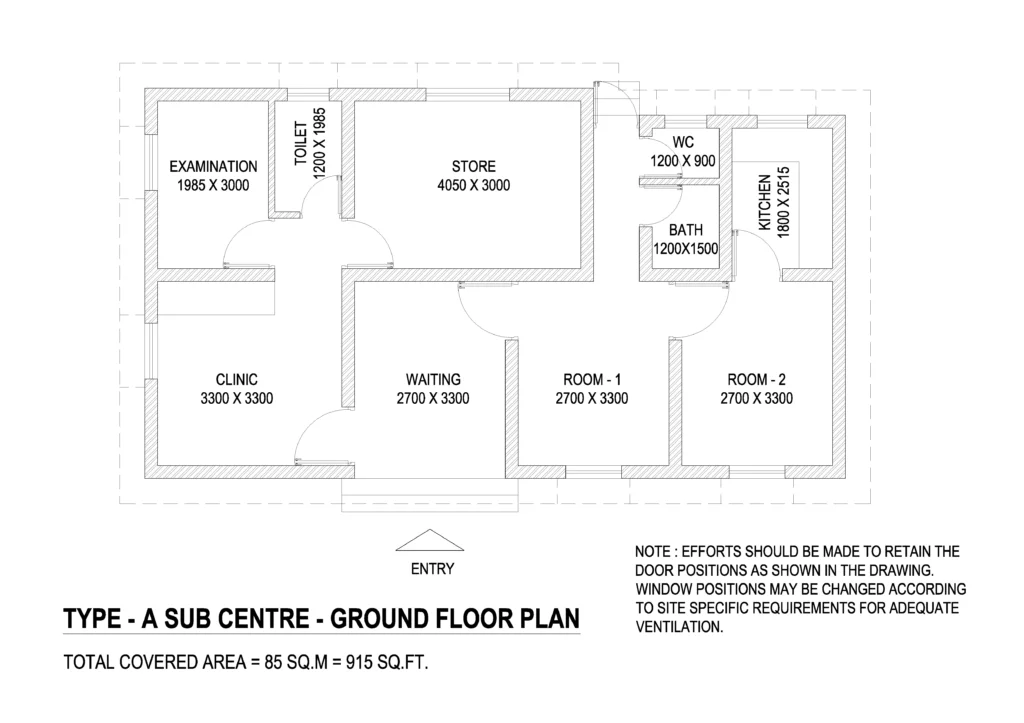
One toilet facility each in labour room ward room and in waiting area (Essential) Residential Accommodation: this should be made available to the Health workers with each one having 2 rooms, kitchen, bathroom and Water Closet (WC). Residential facility for one ANM is as follows which is contiguous with the main Sub-centre area.
- Room – 1 (3.3 m x 2.7 m)
- Room – 2 (3.3 m x 2.7 m)
- Kitchen – 1 (1.8 m x 2.5 m)
- W.C (1.2 m x 9.0 m)
- Bath Room (1.5 m x 1.2 m)
Residential Facility for a minimum of 2 staff and desirably for 3 staff should be provided at Type B (MCH) Sub-centres.
A typical layout plan for Type A Sub- centre with ANM residence having area of 85 square metres and Type B Sub-centre having an additional area of 65 square metres on ground floor and 125 square metres on first floor, with area/space specifications is given Below image.
Signage
- the building should have a prominent board displaying the name of the Centre in the local language at the gate and on the building.
- Prominent display boards in local language providing information regarding the services available and the timings of the Sub-centre should be displayed at a prominent place.
- Visit schedule of “ANMs” should be displayed.
- Suggestion/complaint box for the patients/ visitors and also information regarding the person responsible for redressal of complaints, be displayed. Disaster Prevention Measures against Earthquake, flood and fire (Desirable for all new upcoming facilities)
- Earthquake proof measures – building structure and the internal structure of SC should be made disaster proof especially earthquake proof. Structural and non-structural elements should be built in to withstand quake as per geographical/ state govt. guidelines. Non structural features like fastening the shelves, equipment etc. are as important as structural changes in the buildings.
- SC should not be located in low lying area to prevent flooding.
- Fire fighting equipment – fire extinguishers, sand buckets, etc. should be available and maintained to be readily available when there is a problem.
- The health staff should be trained and well conversant with disaster prevention and management aspects.
Environment Friendly Features
The SC should be, as far as possible, environment friendly and energy efficient. Rain-Water harvesting, solar energy use and use of energy-efficient bulbs/ equipment should be encouraged.
Furniture
Adequate furniture that is sturdy and easy to maintain should be provided to the Sub-centre.
Equipment
the equipment provided to the Sub-centres should be adequate to provide all the assured services in the Sub- centres. this will include all the equipment necessary for conducting safe deliveries at Sub centre (for Type B Sub-centres), home deliveries (for both Type A and Type B), immunization, contraceptive services like IuD insertion, etc.
In addition, equipment for first aid and emergency care, water quality testing, blood smear collection should also be available. Maintenance of the equipment should be ensured either through preventive maintenance/prompt repair of non- functional equipment so as to ensure uninterrupted delivery of services.
A standard mechanism should be in place for the same. Proper sterilization of all equipment and compliance of all universal precautions are to be ensured.
Drugs
The list of drugs that should be available as per the guidelines. Accurate records of stock should be maintained.
Support Services
Laboratory: Minimum facilities of urine Pregnancy testing, estimation of haemoglobin by using a approved Haemoglobin Colour Scale (only approved test strips should be used), urine test for the presence of protein and sugar by using Dipsticks should be available. (Instructions should be followed from the leaflet provided by the manufacturer)
Electricity: Wherever facility exists, uninterrupted power supply has to be ensured for which inverter facility/solar power facility is to be provided. Generator facility is made available at type b Sub centres.
Water: Potable water for patients and staff and water for other use should be in adequate quantity. Towards this end, adequate water supply and water storage facility (over head tank) with pipe water should be made available especially where labour room is attached.
Safe water may be provided by use of technology like filtration, chlorination, etc. as per the suitability of the centre. Water source for Sub-centre be provided by the Panchayat and where there is need a tube well with fitted water pump be provided.
For continuous water supply, States may explore the option of rain water harvesting, solar energy for running the pumps etc.
Telephone: At Type B Sub-centres, landline telephone facility should be provided
Assured Referral linkages: Either through Govt/ PPP model for timely and assured referral to functional PHCs/FRus in case of complications during pregnancy and child birth.
Toilet: toilet facility for use of patients/attendants and Sub-centre Staff must be provided in all Sub-centres. In case of Type B Sub-centre, additional one toilet facility each in labour room and ward room are also to be provided. Regular cleaning of toilets should be ensured.
Waste Disposal
Infection Management and Environment Plan “Guidelines for Health Care Workers for Waste Management and Infection Control in Sub Centres” of Ministry of Health and Family Welfare, Government of India are to be followed.
Standards for Deep burial Pit as per bio-Medical Waste (Management and Handling) Rules, 1998 are given at Standards for Deep burial Pit
Record Maintenance and Reporting
Proper maintenance of records of services provided at the Sub-centres and the morbidity/mortality data is necessary for assessing the health situation in the Sub-centre area.
In addition, all births and deaths under the jurisdiction of sub- centre should be documented and sex ratio at birth should be monitored and reported.
Monitoring Mechanism
Internal mechanisms: Supportive supervision and Record checking at periodic intervals by the Male and Female Health supervisors from PHC (at least once a week) and by MO of the PHC (at least once in a month) etc.
External mechanisms: Sub-centres will be under the oversight of Gram Panchayats.
A detailed Facility Survey Format is also given to monitor periodically whether the Sub centre is up-to the level of Indian Public Health Standards (IPHS).
PRI should also be involved in the monitoring. the following may be monitored:
- Access to service (equity). Location of Sub-centres ensuring it to be safe to female staff and centrally located, well in side the inhabited area of the village.
- Registration and referral procedures; promptness in attending to clients; transportation of emergency maternity cases etc.
- Management of untied fund for the improvement of services of the Sub- centre
- Staff behaviour
- Other facilities: waiting space, toilets, drinking water in the Sub-centre building.
Quality Assurance and Accountability
This can be ensured through regular skill development training/Continuing Medical Education (CME) of health workers (at least one such training in a year), as per guidelines of NRHM.
In order to ensure quality of services and patient satisfaction, it is essential to encourage community participation. to ensure accountability, the Citizens’ Charter should be available in all Sub-centres.