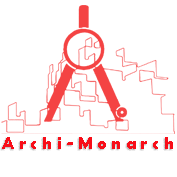
An operating unit in a healthcare facility refers to the physical and functional space where surgical procedures are performed.
Commonly known as the Operating Room (OR) or Surgical Suite, this unit encompasses not only the surgical theater itself but also adjoining areas such as pre-operative (pre-op) zones, post-anesthesia care units (PACU), sterile processing rooms, and surgical storage areas.
It is a highly specialized environment that must support precision, sterility, and rapid responsiveness.
Why Effective Operating Unit Design Matters
The design of the operating unit has a direct impact on patient safety, staff efficiency, and clinical outcomes. Well-planned layouts help:
- Minimize infection risks through sterile zoning and effective airflow systems.
- Improve staff workflow by ensuring seamless access to tools, technology, and support areas.
- Enhance communication and coordination among multidisciplinary surgical teams.
- Reduce procedure times by optimizing the positioning of equipment and supplies.
- Support patient privacy and dignity throughout the surgical process.
Ultimately, a thoughtfully designed operating unit saves lives, reduces complications, and increases the overall efficiency of healthcare delivery.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
The Operating Unit provides a safe and controlled environment for the operative care of patients undergoing diagnostic/ surgical procedures under anaesthesia and peri-operative care including post procedure recovery.
2) Planning of Operating unit
i) Operational Models
Operation models include the following options:
Integrated ambulatory care model
This is a dedicated unit where patients access surgical and/or medical procedures and other complementary services on a planned day-only basis.
Peri-operative model
In this model patients have planned surgery and are admitted as a day-only or day-of-surgery admission in a dedicated facility. Surgery and 1st stage recovery is undertaken in the Operating Unit.
Day-only cases are then transferred back to the facility for pre-discharge care. Day-of-surgery admissions may be transferred to an inpatient unit following recovery.
Short stay surgery model
This is a dedicated unit where patients have planned surgery as a day-only or overnight admission; patients are transferred to the Operating Unit for surgery and 1st stage recovery, and then returned to the facility.
Post-operative stay is usually less than 48 hours.
Specialist surgey model
This model provides for a single specialty or compatible specialties such as ophthalmology, plastic surgery or urology. Patients are admitted and discharged on a day-only basis.
ii) Planning Models
The Operating Unit shall be located and arranged to prevent non-related traffic through the suite. The number of Operating Rooms and Recovery beds and the sizes of the service areas shall be based on the service plan and expected surgical workload.
The size, location, and configuration of the surgical suite and support service departments shall reflect the projected case load and service plan of the Unit.
A number of planning models may be adopted including:
Single corridor
The single corridor model involves travel of all supplies (clean and used) as well as patients (pre and post operative) in one main corridor. There is ongoing debate as to the suitability of this approach.
However, this option is considered suitable provided:
- the main corridor is sufficiently wide in order to permit separation of passage of goods and services;
- handling of clean supplies and waste is carefully managed to avoid cross contamination A major disadvantage of this planning model is that a patient awaiting surgery may be exposed to post operative patients
Dual corridor or Race track
The Dual Corridor or ‘Race Track’ model allows for all the Operating rooms to be accessed from an external corridor for patients and directly from a central Set Up/Sterile Stock Room for sterile goods. This model aims to separate ‘dirty’ from ‘clean’ traffic by controlling the uses of each corridor.
In this design, there must not be cross traffic of staff and supplies from the decontaminated / soiled areas to the sterile / clean areas.
In this model, stock and staff can be concentrated in one location, preventing duplication of equipment stock and staff.
Clusters of operating rooms
In this model Operating Rooms may be clustered according to specialty, with a shared Sterile Stock and Set-Up Room for each group or cluster.
Disadvantages of this model include:
- additional corridor and circulation space required for corridors around clusters of rooms, which reduces the available space for stock;
- potential duplication of stock and additional staff requirements may result in increased operating costs
Dedicated theatres with fixed or mobile equipment
In this model Operating rooms are dedicated to specific types of surgery such as hybrid operating/ imaging rooms, urology, vascular, neurology or other specialties requiring specific equipment.
This may be beneficial in larger suites where the case volume justifies specialisation, however, smaller suites may favour flexibility of Operating Room use. Fixed equipment can preclude the multifunctional use of the room.
TSSU/ CSSU
The Operating Unit is a major user of sterile stock and the location of the instrument processing area and sterile stock is of high importance. There are two main options available for supply of sterile stock to the Operating Unit:
- a dedicated TSSU (Theatre Sterile Supply Unit) serving only the Operating Unit
- a CSSU (Central Sterile Supply Unit) that also serves other areas of the hospital.
The TSSU may be located within the Operating Suite or externally. It is preferable to locate the TSSU adjacent with direct access to the Operating Suite.
The TSSU may also be located on another floor of the building connected by dedicated clean and used goods lifts.
The CSSU may be located in a service zone of the hospital. There is a strong functional link between the CSSU and the Operating Unit; efficient transport of stock to and from each unit will require careful planning.
iii) Functional Areas
The Operating Unit consists of the following functional areas:
- Admissions and Reception Area for receival and admission of patients to the Unit, with general overseeing of day to day operations, control of entry and exit from the Unit and completion of general administrative tasks
- Holding areas for holding and management of patients prior to their operation or procedure
- Operating Rooms area where procedures are carried out
- Support Areas including storage and management of stock and sterile supplies, disposal of waste and sterilisation of smaller items
- Recovery Areas where patients are assisted through the process of recovering from the effects of anaesthetic
- Administrative and Staff Areas including Change Rooms, Staff Room, Offices and administrative space for clinical staff.
Dental surgery
In addition to the standard operating room equipment and services (refer to Standard Component Operating Room), items considered essential for dental procedures are as follows:
- One compressed dental air outlet situated close to the service panels for medical gases, suction and electrical outlets, with the provision of a regulated bottle of appropriate compressed air as emergency backup or secondary use
- Facilities for dental X-ray.
Laboratory areas
Depending on the service plan and unit policy, an area for preparation and examination of frozen sections may be provided.
This may be part of the general Pathology Laboratory if immediate results are obtainable without unnecessary delay in the completion of surgery.
Staff amenities
Appropriate Change Rooms, toilet and showers shall be provided for male and female personnel (nurse, doctors and technicians) working within the Operating Unit.
The Change Rooms shall contain adequate lockers, showers, toilets, handbasins and space for donning surgical attire and booting.
Staff Change Rooms shall be arranged to encourage a one-way traffic pattern so that personnel entering from outside the surgical suite can change and move directly into the Operating Unit.
Alternatively, the entrance to the Change Rooms may be planned in direct view of a Staff Station at the entrance to the Operating Unit. The Change Room entrance door shall be provided with locks or electronic access devices to prevent the entry of unauthorised persons into the Operating Unit.
Notes:
- It is desirable but not mandatory to increase the number of facilities for female change rooms by approximately 30%
- In male change rooms 50% of toilets may be replaced with urinals
- Warm air hand dryers shall be avoided
Flash sterilising facilities
A Flash Steriliser should be located in the unit, however, the use of this method of sterilising should be restricted to situations where a single instrument has been dropped and there is no sterile duplicate available.
Flash sterilising is not suitable for processing of cannulated, complex instruments, suction and other tubing, textiles, paper or liquids.
Storage
Adequate Equipment Store room/s for equipment and supplies used in the Operating Unit shall be provided. Equipment Stores shall be provided at the minimum rate of 10 m2 per Operating Room.
Note:
- Store Rooms do not necessarily require doors.
- Store Rooms are best designed in an elongated rectangular shape to allow easy access to all items.
- The design of the Operating Unit should allow for ease of access to the storage areas for delivery of Operating Unit consumables. Controlled access from an external corridor is highly desirable.
Mobile Equipment Bays shall be provided for equipment such as portable X-ray equipment, stretchers, trolleys, warming devices and mobile equipment.
Mobile Equipment Bays shall comply with Standard Components and be provided at the minimum quantity of one per operating room. Equipment Bays are best designed as elongated rectangular shapes and may be combined for space efficiency.
Biomedical store / workshop
An area for testing operating equipment may be included in the Operating Unit. This room may be collocated with a General Store, or a dedicated room for this purpose may be necessary.
A direct corridor access to this room is recommended, with controlled access to the remainder of the Operating Unit
iv) Functional Relationships
The Operating Unit requires close relationships with the following areas, particularly for urgent cases:
- Emergency Unit
- Intensive Care Units
- Obstetric Unit
- Helipad
Links between these Units and the Operating Unit should be rapid, direct and discreet; transit of severely ill patients to and from the Unit through public corridors should be avoided.
The Operating Unit has a direct operation link with the following Units:
- Peri-operative Unit/ Day Surgery
- TSSU/ CSSU
Other Units that have a close relationship include:
- Pathology;
- Imaging
- Obstetric/ Birthing Unit for Caesarean Section procedures
3) Design of Operating unit
i) Environmental Considerations
Natural light
The need for an external view from the Operating Room is an important consideration. Provision of windows need to consider the following:
- vision from the Operating Room could be through a corridor, set up area or directly to the external environment
- many procedures require black-out
- there are heating, cooling and shading implications for windows in the Unit located on the outside of the building that may have an impact on the recurrent costs for maintenance and cleaning
- viewing windows from a corridor to the Operating Room can be useful for supervision and training purposes
- windows to Recovery, Staff Lounge and TSSU areas where staff spend a majority of their time, should be given a high priority.
ii) Finishes
Operating Units shall have the following finishes:
- floors that are smooth, non-slip impervious material laid in a continuous washable material and graded where necessary to fall to floor waste; floor material that resists staining is recommended
- wall finishes which are seamless, impervious and washable
- ceilings which are smooth and impervious
- intersections of walls and architraves to be rendered watertight junctions.
In all areas where patient observation is critical such as Operating Room/s, Anaesthetic Room/s, Recovery Area/Room, Holding Area/Room, colours shall be chosen that do not alter the observer’s perception of skin colour.
iii) Infection Control
Infection control issues are paramount in the Operating Unit and require careful attention to planning models and separation of clean and dirty workflows. Refer to Infection Control.
iv) Safety and Security
Access control is required to the patient and staff entry areas of the Operating Unit. Limiting the number of entries and locating the Reception area with direct overview of entry areas is highly desirable.
v) Building Services Requirements
Medical gases
Main storage of medical gases must be outside the facility and reticulated internally to gas outlets. Provision shall be made for additional separate storage of reserve gas cylinders necessary to complete at least one day’s procedures.
4) Components of the Unit
The Operating Unit will consist of a combination of Standard Components and Non-Standard Components. Provide Standard Components to comply with details in Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets.
i) Non Standard Components
Perfusion room
Description and Function – The Perfusion Room is for the preparation of perfusion equipment, and where set-up for cardiac procedures is undertaken.
Location and Relationships – The room will be located in close proximity to the Cardiac Operating Room/s and adjacent to a Perfusion Store.
Considerations – Room requirements may include:
- Heavy duty shelving for storage of perfusion fluids and equipment
- Computer workstation for a perfusion technician including power and data outlets
- Handwashing basin Type B with paper towel and soap fittings
- Bench, sink and cupboard unit for servicing of the perfusion machine
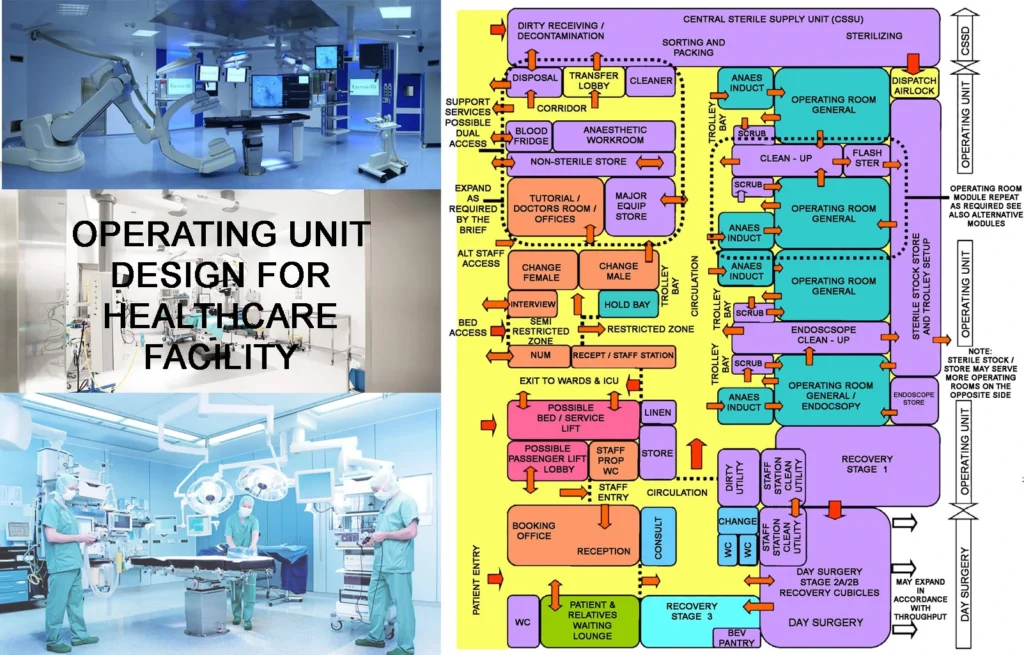
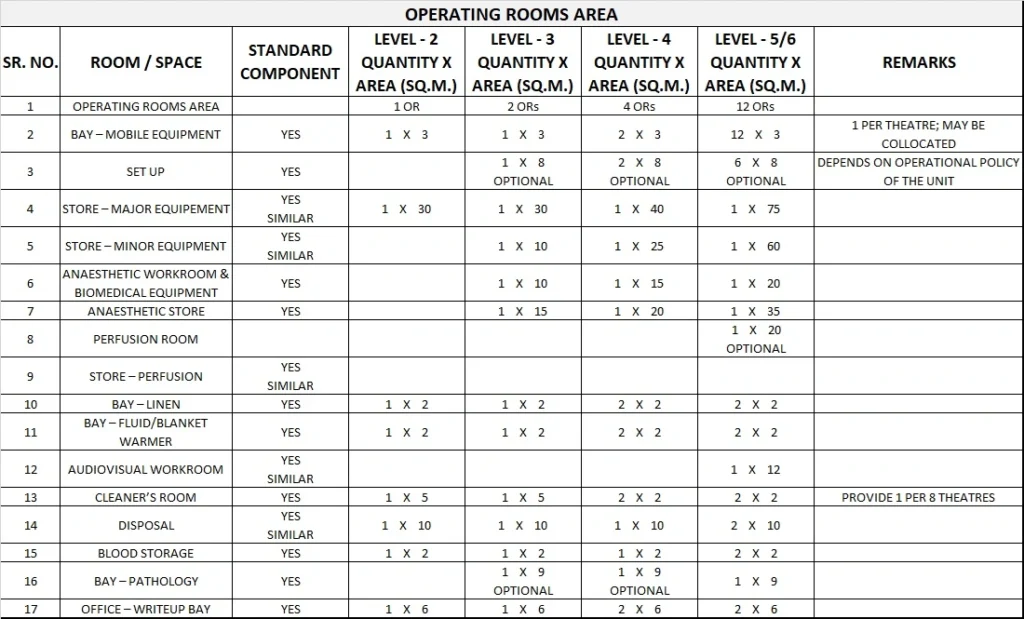
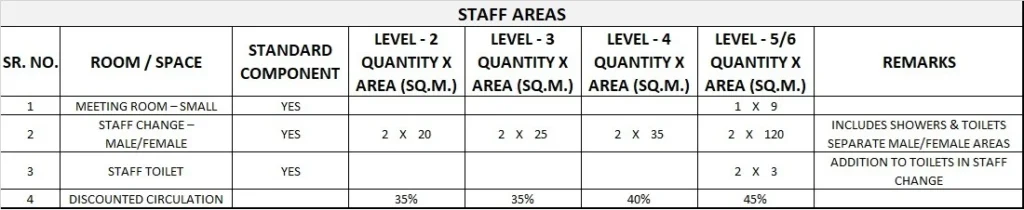
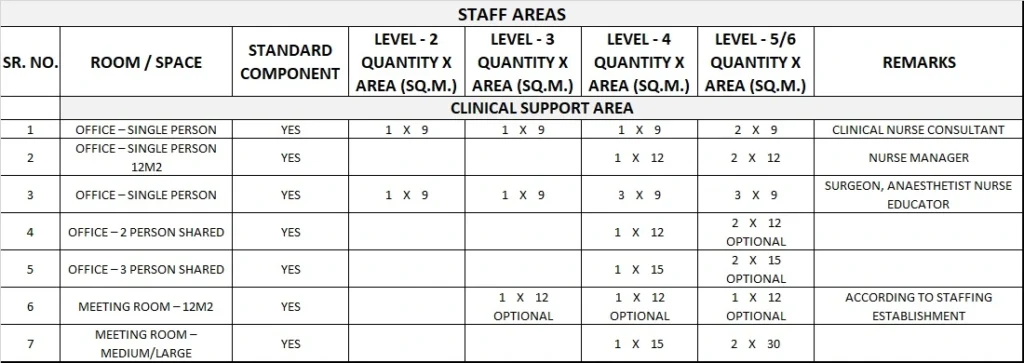
5) Schedule of Accommodation
Operating Unit Generic Schedule of Accommodation
Schedule of Accommodation for an Operating Unit for Level 2-6

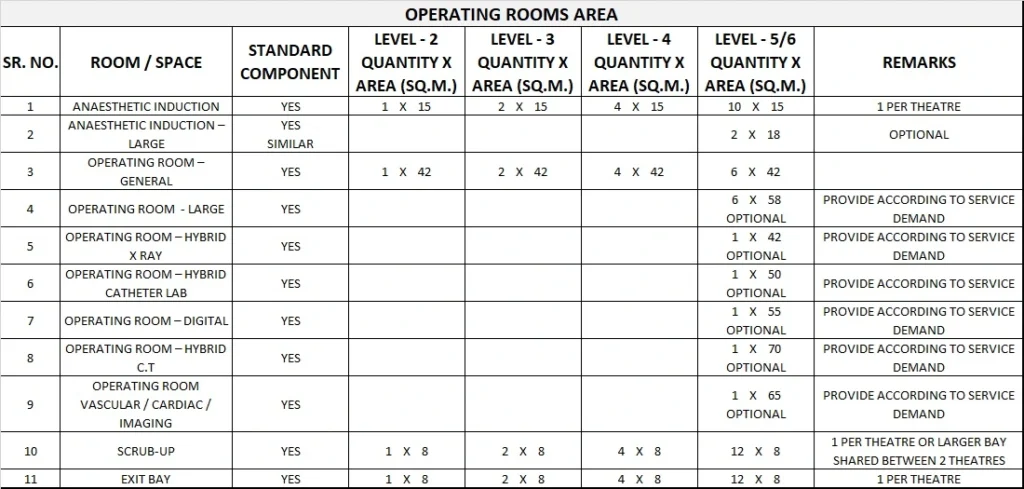


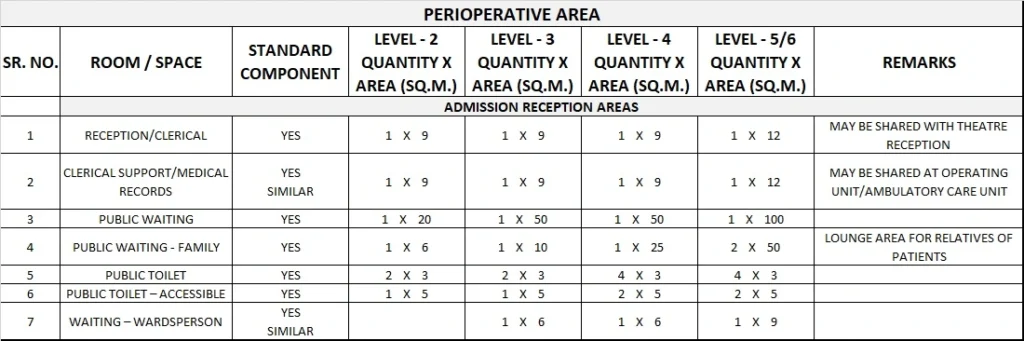
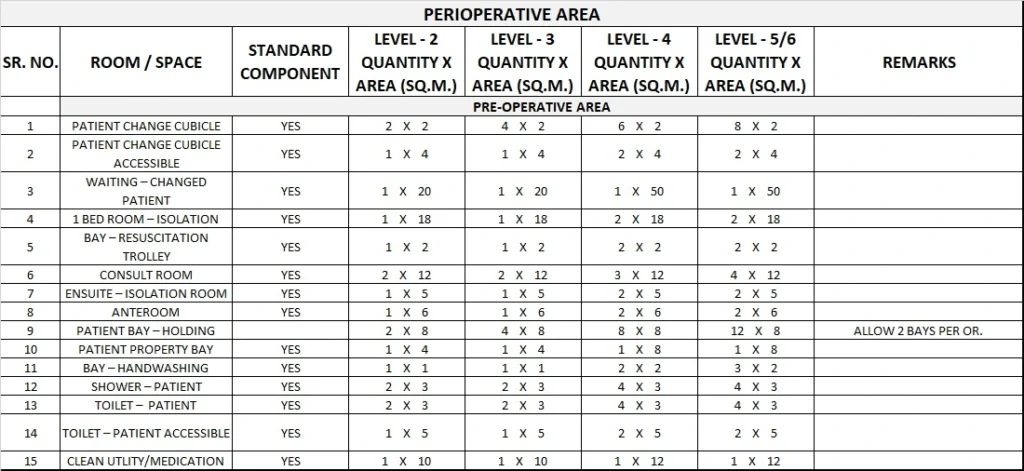
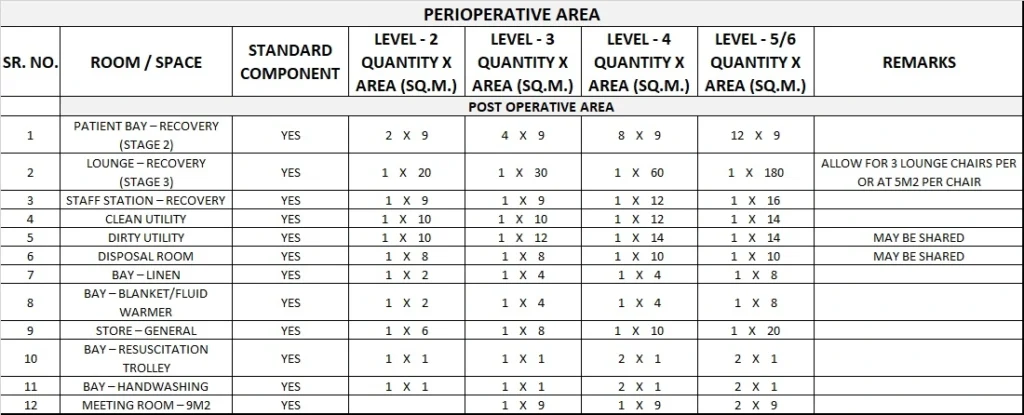
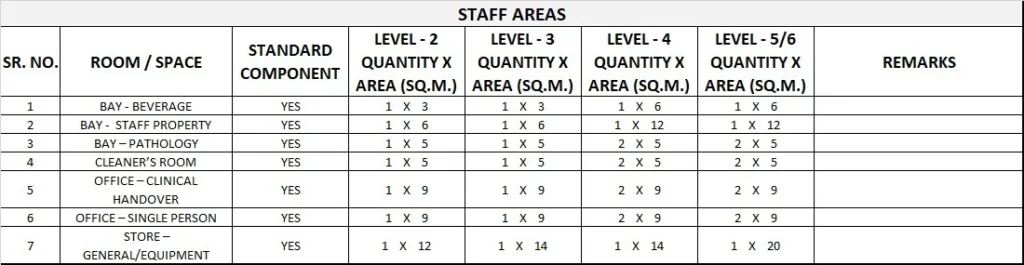

Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
6) Functional Relationship Diagram
Operating Unit Functional Relationship Diagrams
The relationships between the various components within an Operating Unit are best described by functional relationships diagrams.
The requirements for infection control and patient management result in a number of planning ‘models’ that have proved successful through numerous built examples and many years of practice.
Most Operating Unit plans are a variation of one of these ‘models’.
A plan substantially based on one of these diagrams is ‘deemed to satisfy’ the requirements of these Guidelines. A plan that is significantly different to these diagrams should be carefully examined against all the individual requirements of these Guidelines, especially those of Infection Control to determine if it is acceptable.
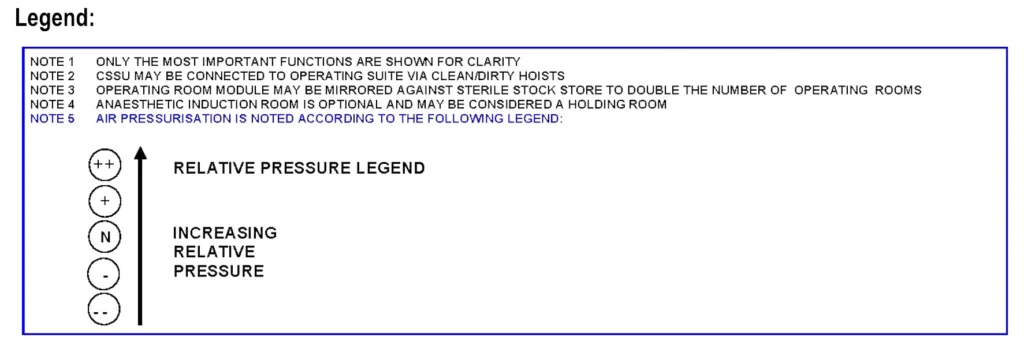
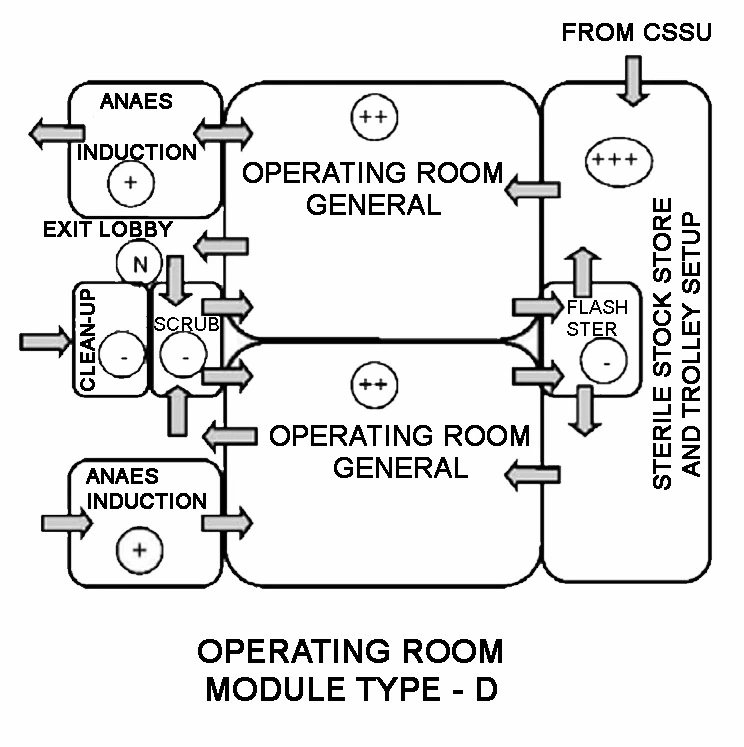
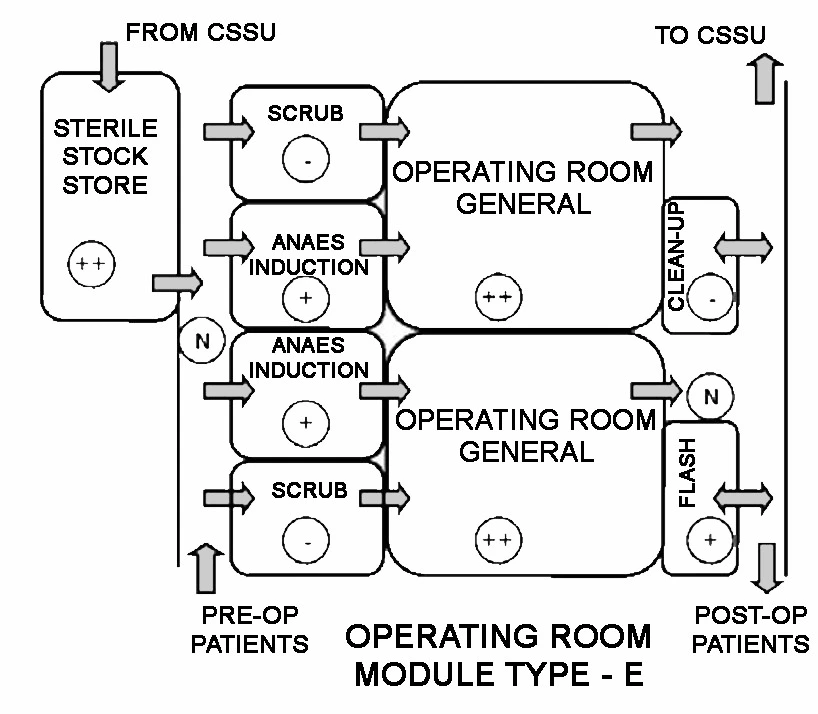
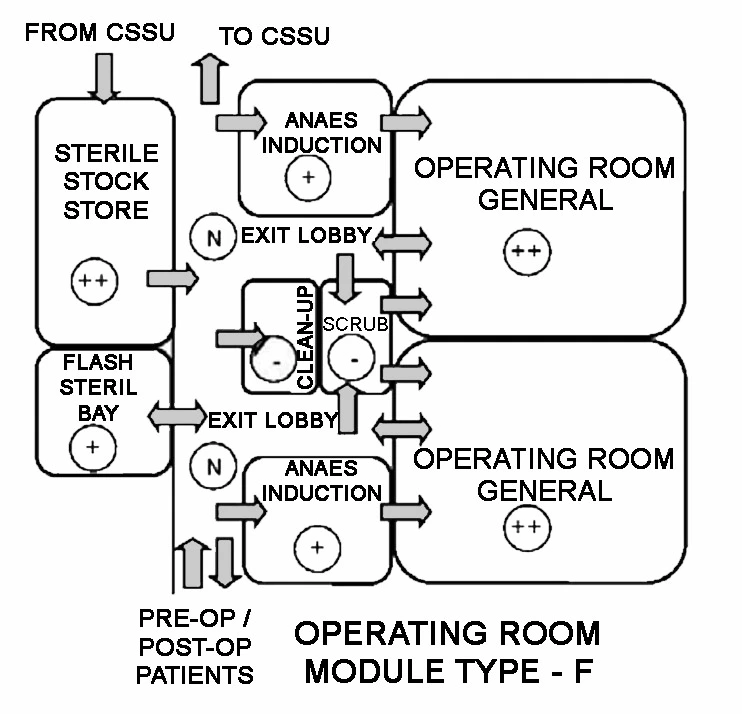
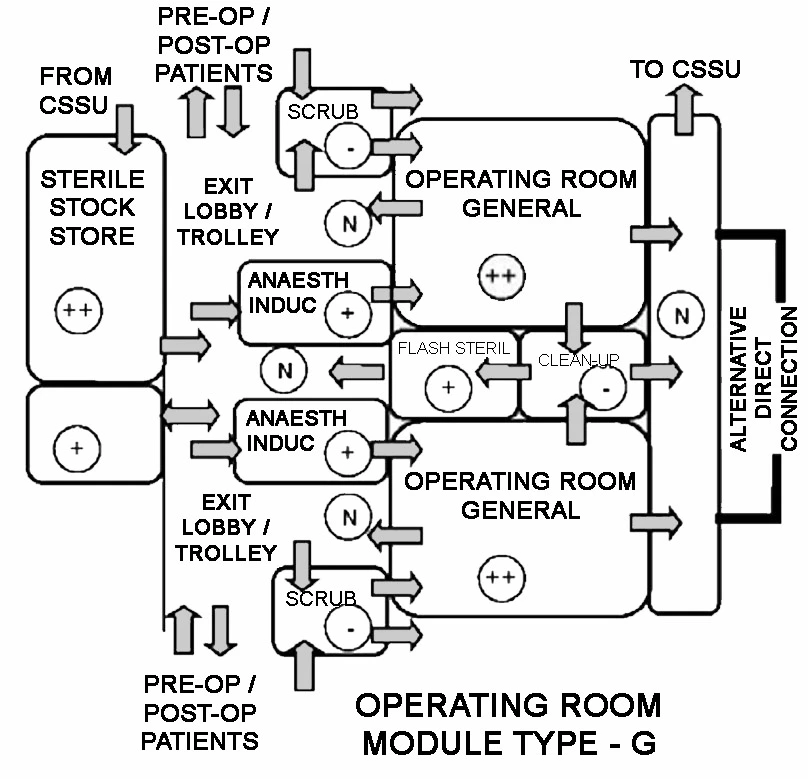
In reviewing and using the enclosed Operating Unit flow diagrams, designers should carefully consider a number of issues:
- Each flow diagram represents a method of managing the patient access, clean/dirty flow, air pressurisation, sterilisation of dropped instruments etc.
- The diagrams are different but each addresses the issues involved in a satisfactory manner. Each option may suit a different management mode or building configuration.
- Designers are strongly cautioned against creating hybrid options by combining features of various diagrams. This may result in wrong clean/ dirty flows or other unacceptable features. If in doubt, designers should seek advice from specialist Operating Room consultants and Infection Control nurses.
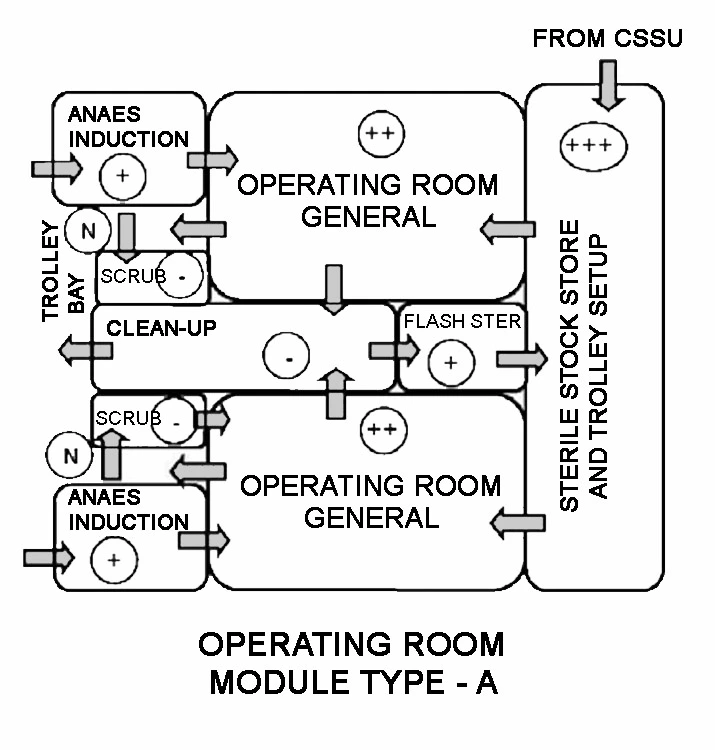
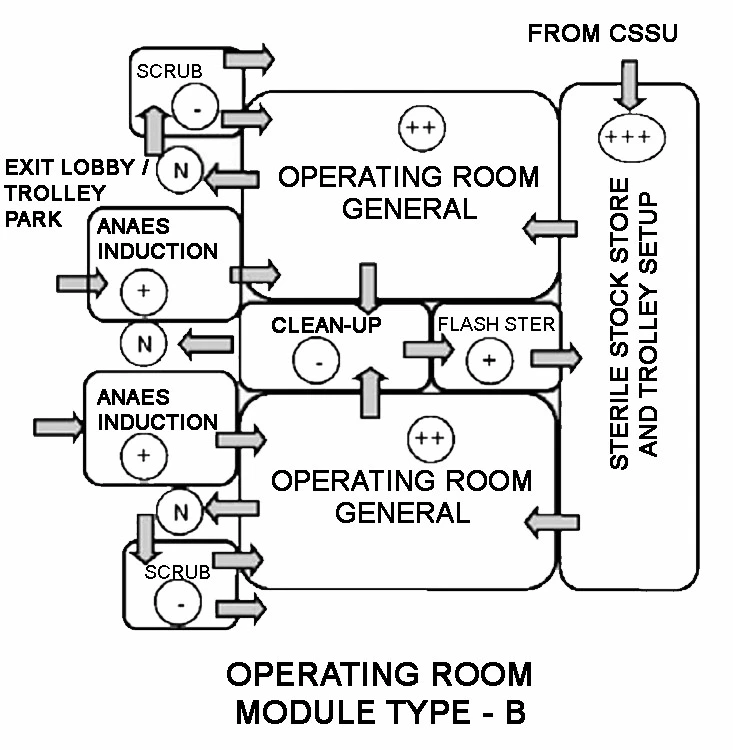
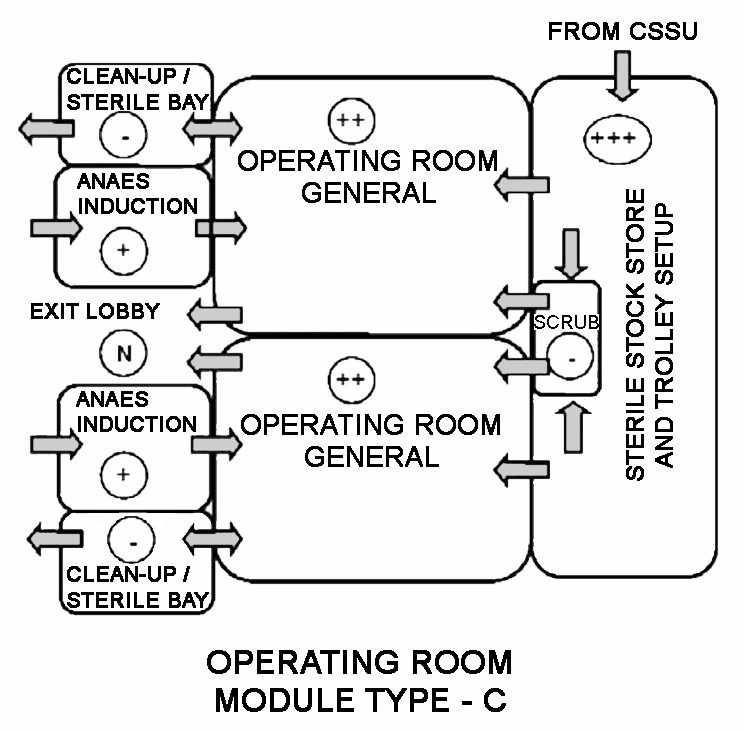
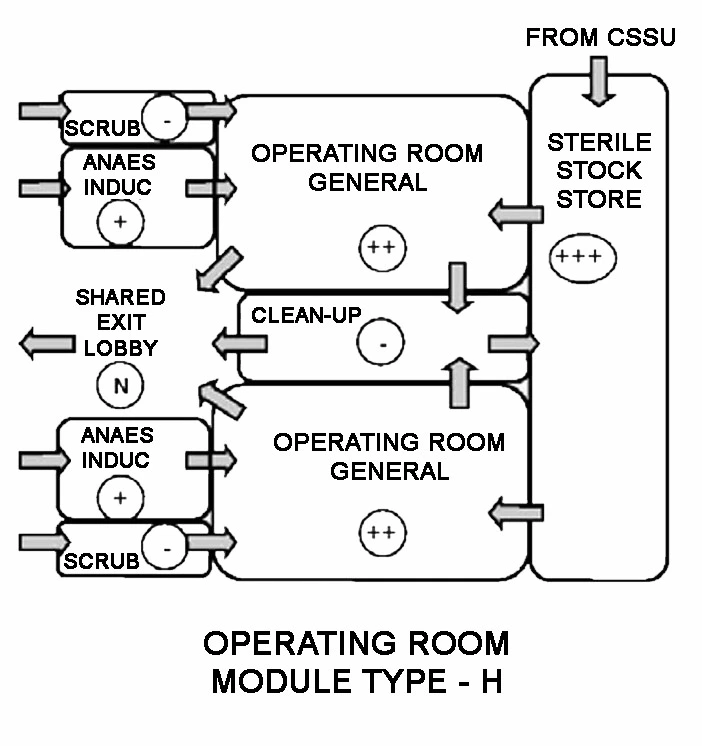
The functional relationship diagrams in Enclosures 1 and 2 show base linear models. The models can be stretched to create the number of Operating Rooms desired.
The support facilities required also grow with the number of Operating Rooms. Each module includes the configuration of:
- Operating Rooms
- Anaesthetic Induction Rooms
- Scrub Bays or Rooms
- Sterile Stock Store / Set-up Room
- Clean-up Room
- Flash Sterilising Bay
Enclosure 1: Single corridor model
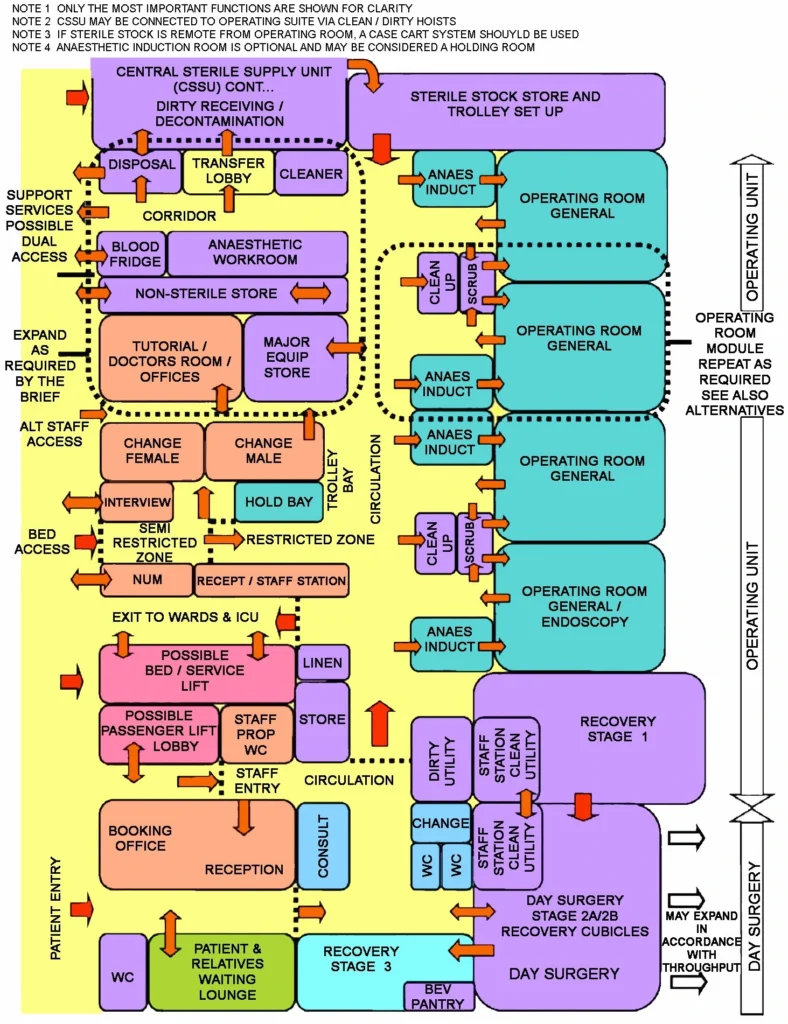
Enclosure 2 : Dual corridor model
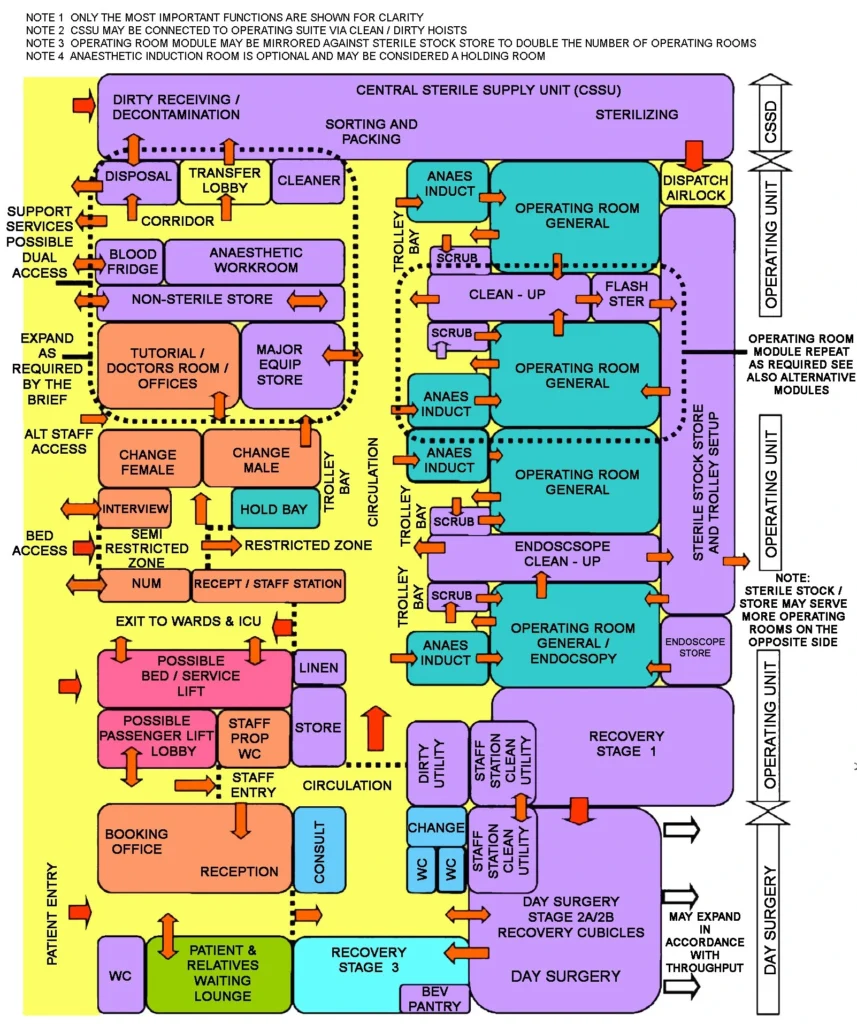
Enclosure 3: Operating room modules A TO H with air pressurisation