Inpatient accommodation units serve as the heart of any healthcare facility, providing a dedicated space where patients receive continuous medical care and recover from illnesses, surgeries, or treatments.
These units typically include patient rooms, bathrooms, nurse stations, and family spaces, all designed to ensure patients’ comfort, privacy, and safety. As healthcare evolves, inpatient unit design is becoming increasingly patient-centered, reflecting a shift toward holistic healing environments that support both physical and emotional well-being.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
The prime function of the Inpatient Unit is to provide appropriate accommodation for the delivery of health care services including diagnosis, care and treatment to inpatients.
The Unit must also provide facilities and conditions to meet the needs of patients and visitors as well as the workplace requirements of staff.
The Inpatient Accommodation Unit is for general medical and surgical patients. In larger health facilities this Unit includes specialist medical and surgical patients, for example, cardiac, neurology/ neurosurgery, integrated palliative care and obstetric patients. Patients awaiting placement elsewhere may also be accommodated in this type of facility.
2) Planning of Inpatient Accommodation Unit
i) Models of Care
Models of Care for an Inpatient Unit may vary dependent upon the patients’ acuity and numbers of, and skill level of the nursing staff available. Examples of the models of care that could be implemented include:
- patient allocation
- task assignment
- team nursing
- case management
- primary care (comprehensive range of generalist services by multidisciplinary teams that include not only GPs and nurses but also allied health professionals and other health workers) or
- a combination of these
The physical environment should permit of a range of models of care to be implemented, allowing flexibility for future change.
Levels of care
The levels of care will range from highly acute nursing and specialist care (high dependency), with a progression to intermediate care prior to discharge of transfer (self care). Patients requiring 24 hour medical intervention or cover will generally not be nursed or managed within a general inpatient unit.
ii) Planning Models
Bed numbers and complement
Each Inpatient Unit may contain up to 32 patient beds and shall have Bedroom accommodation complying with the Standard Components.
For additional beds up to 16 as an extension of a standard 32 bed Unit, this may be permitted with additional support facilities in proportion to the number of beds, for example 1 extra Sub Clean Utility, Sub Dirty Utility and storage.
For additional beds of more than 16, additional support facilities for a full unit (32 beds) will be required, located to serve the additional beds. The preferred maximum number of beds in an acute Inpatient Unit in Maternity or Paediatric Units is 20-25 beds.
A minimum of 10 % of the total bed complement may be provided as Single Bedrooms in an Inpatient Unit used for overnight stay for Isolation of patients. The current trend is to provide a greater proportion of single bed rooms largely for infection control reasons.
Swing Beds
For flexibility and added options for utilisation it may be desirable to include provisions for Swing Beds. This may be a single bed, a group of beds that may be quickly converted from one category of use to another. An example might be long-stay beds which may be converted to acute beds.
At any given time, swing beds are part of an Inpatient Unit in terms of the total number of beds and the components of the unit. For example:
- Ward A + Swing Beds = One Inpatient Unit as per these Guidelines.
- Alternatively: Ward B + the same Swing Beds = One Inpatient Unit as per these Guidelines.
Facility design for swing beds will often require additional corridor doors and provision for switching patient/ nurse call operation from one Staff Station to another. Security is also an issue, for example, converting General/Medical beds to Paediatric beds.
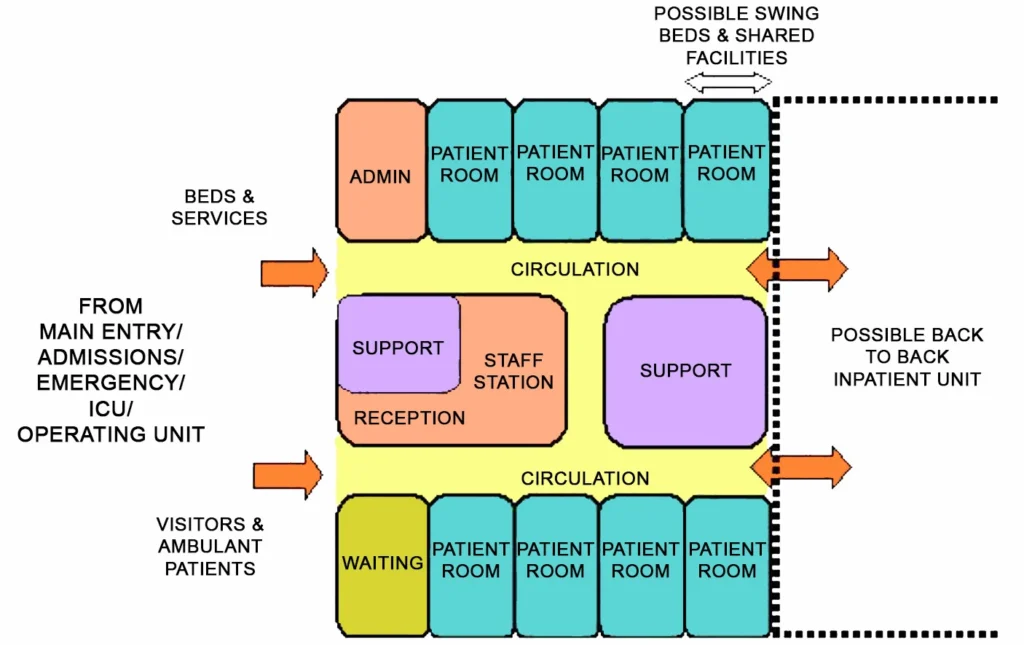
Unit planning options
There are a number of acceptable planning options for Inpatient Units including:
- Single Corridor; Patient and support rooms are clustered along a single corridor
- Double Corridor – racetrack; patient rooms are located on the external aspects of the space and support rooms are clustered in the central areas in a racetrack configuration
- Combinations: – L, T & Y shaped corridors, patient rooms are located along external aspects, support areas may be located in a central core area
iii) Functional Areas
The Inpatient Accommodation Unit will comprise the following Functional Areas or zones:
- Patient Areas – areas where patients are accommodated or facilities specifically serve patients
- Staff Areas – areas accessed by staff, including utility and storage areas
- Shared Areas – areas that may be shared by two or more Inpatient Units
iv) Functional Relationships
External
Principal relationships with other Units include:
- Easy access from the Main Entrance of a facility
- Inpatient Units must not be located so that access to one Unit is via another
- Ready access to diagnostic facilities such as Medical Imaging and Pathology
- Ready access to Emergency and Critical Care Units
- Surgical Units require ready access to Operating/ Day Procedures Units
- Ready access to staff amenities.
Internal
Optimum internal relationships include:
- Patient occupied areas as the core of the unit
- The Staff Station and associated areas need direct access and observation of Patient Areas
- Utility and storage areas need ready access to both patient and staff work areas
- Public Areas should be on the outer edge of the Unit
- Shared Areas should be easily accessible from the Units served
3) Design of Inpatient Accommodation Unit
i) Environmental Considerations
Acoustics
The Inpatient Unit should be designed to minimise the ambient noise level within the unit and transmission of sound between patient areas, staff areas and public areas.
Consideration should be given to location of noisy areas or activity away from quiet areas including patient bedrooms and selection of sound absorbing materials and finishes.
Acoustic treatment will be required to the following:
- patient bedrooms,
- interview and meeting rooms
- consult rooms
- staff rooms
- toilets and showers
Please refer to “ACOUSTICS FOR HEALTHCARE FACILITY”
Natural light
The use of natural light should be maximised throughout the Unit. Natural light must be available in all bedrooms.
Observation and Privacy
The design of the Inpatient Unit needs to consider the contradictory requirement for staff visibility of patients while maintaining patient privacy. Unit design and location of staff stations will offer varying degrees of visibility and privacy. The patient acuity including high dependency, elderly or intermediate care will be a major influence.
Factors for consideration include:
- use of windows in internal walls and/or doors
- location of beds that may affect direct staff visibility
- provision of bed screens to ensure privacy of patients undergoing treatment;
- location of sanitary facilities to provide privacy for patients while not preventing observation by staff.
ii) Space Standards and Components
Room Capacity and Dimensions
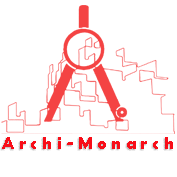
Maximum room capacity shall be eight beds, although six is preferred. Minimum dimensions, excluding such items as ensuites, built-in robes, alcoves, entrance lobbies and floor mounted mechanical equipment shall be as follows:

Minimum room dimensions are based on overall bed dimensions (buffer to buffer) of 2250 mm long x 1050 mm wide. Minor encroachments including columns and hand basins that do not interfere with functions may be ignored when determining space requirements
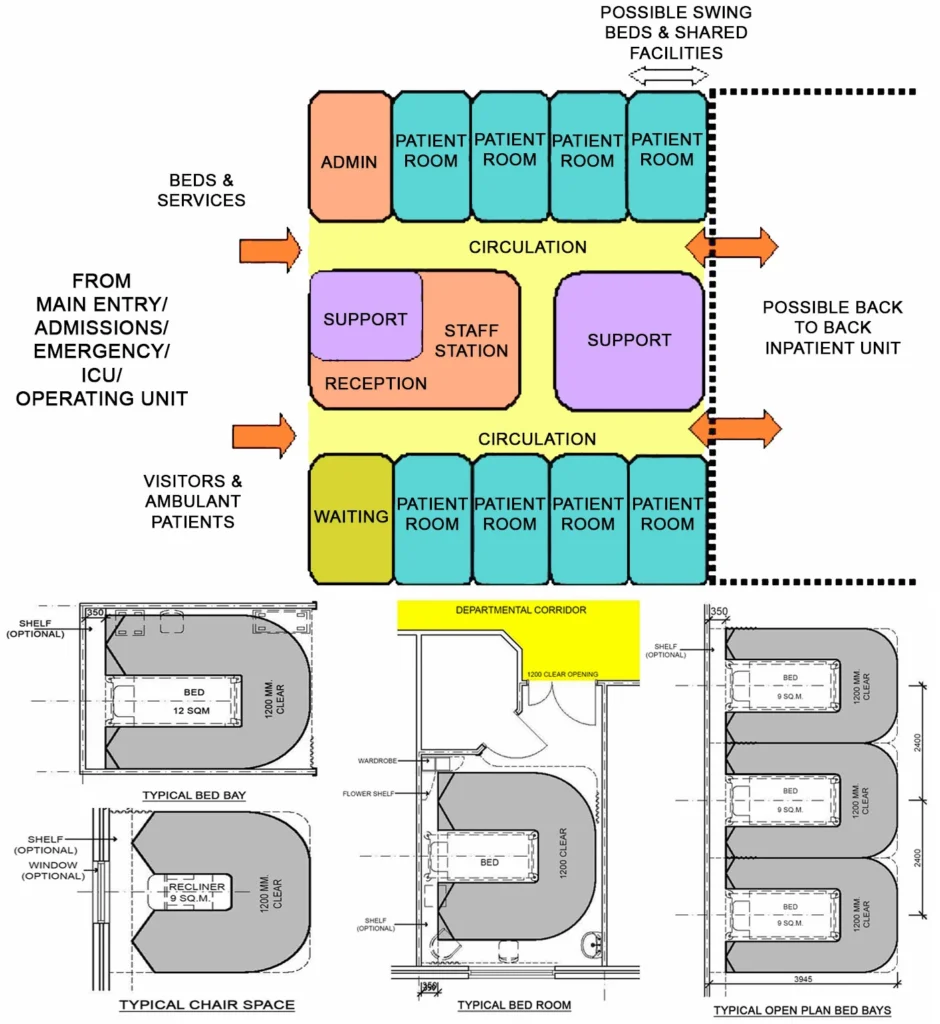
Bed spacing / Clearances
Bed dimensions become a critical consideration in ascertaining final room sizes. The dimensions noted in these Guidelines are intended as minimums and do not prohibit the use of larger rooms where required.
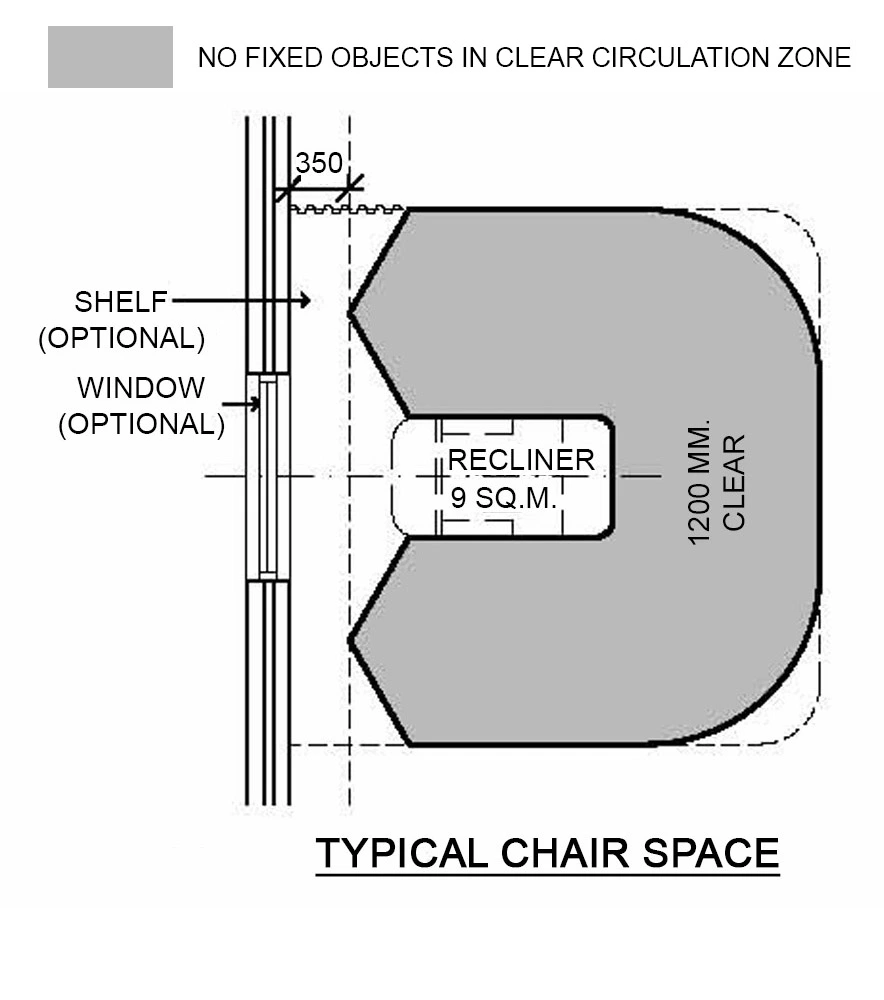
In bed rooms there shall be a clearance of 1200 mm available at the foot of each bed to allow for easy movement of equipment and beds. This is represented diagrammatically below:


In multiple-bed rooms, the minimum distance between bed centre lines shall be mm. Paediatric bedrooms that contain cots may have reduced bed centres, but consideration must be given to the spatial needs of visiting relatives. To allow for more flexible use of the room the 2400 mm centre line is still recommended. Consider allowing additional floor area within the room for the children to play.
The clearance required around beds in multiple-bed rooms and chair spaces is represented diagrammatically below:
iii) Access, Mobility & OH&S (Occupational Health & Safety)
Patient wheelchair access bedrooms and ensuites should enable normalisation of activity for wheelchair dependant patients, as opposed to patients who are in a wheelchair as a result of their hospitalisation.
iv) Infection Control
Hand Basins
Hand-washing facilities shall not impact on minimum clear corridor widths. At least one is to be conveniently accessible to the Staff Station. Handbasins are to comply with Standard Components – Bay – Hand-washing and Part D – Infection Control.
Isolation Rooms
At least one ‘Class S – Standard’ Isolation Room shall be provided for each 32 bed Inpatient Unit. At least one ‘Class N – Negative Pressure’ Isolation Room shall be provided for each 100 beds in facilities of level 4 and above. These beds may be used for normal acute care when not required for isolation.
v) Safety and Security
An Inpatient Unit shall provide a safe and secure environment for patients, staff and visitors, while remaining a non-threatening and supportive atmosphere conducive to recovery.
The facility, furniture, fittings and equipment must be designed and constructed in such a way that all users of the facility are not exposed to avoidable risks of injury.
Security issues are important due to the increasing prevalence of violence and theft in health care facilities.
The arrangement of spaces and zones shall offer a high standard of security through the grouping of like functions, control over access and egress from the Unit and the provision of optimum observation for staff. The level of observation and visibility has security implications
Drug Storage
Each Inpatient Accommodation Unit shall have a lockable storage area or cupboard containing:
- Benches and shelving
- Lockable cupboards for the storage of restricted substances
- A lockable steel cabinet for the storage of drugs of addiction
- A refrigerator, as required; to store restricted substances, it must be lockable or housed within a lockable storage area
- Space for medication trolley
Note: Storage for dangerous drugs must be in accordance with the relevant legislation.
vi) Finishes
Finishes including fabrics, floor, wall and ceiling finishes, should be selected with consideration to infection control, ease of cleaning and fire safety, while avoiding an institutional atmosphere.
In areas where clinical observation is critical such as bedrooms and treatment areas, colour selected must not impede the accurate assessment of skin tones.
vii) Fixtures & Fittings
Bed Screens
In multiple-bed rooms, visual privacy from casual observation by other patients and visitors shall be provided for each patient. The design for privacy shall not restrict patient access to the entrance, toilet or shower.
Curtains / Blinds
Each room shall have partial blackout facilities (blinds or lined curtains) to allow patients to rest during the daytime.
viii) Building Services Requirements
Information Technology / Communications
Unit design should address the following Information Technology/ Communications issues:
- Paperless records
- Hand-held computers
- PACS
- Paging and personal telephones replacing some aspects of call systems
- Data entry including scripts and investigation requests
- Bar coding for supplies and X-rays / Records.
Nurse Call
Hospitals must provide an electronic call system that allows patients and staff to alert nurses and other health care staff in a discreet manner at all times.
4) Components of the Unit
Standard Components
The Inpatient Unit will consist of Standard Components which must comply with details in the Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets
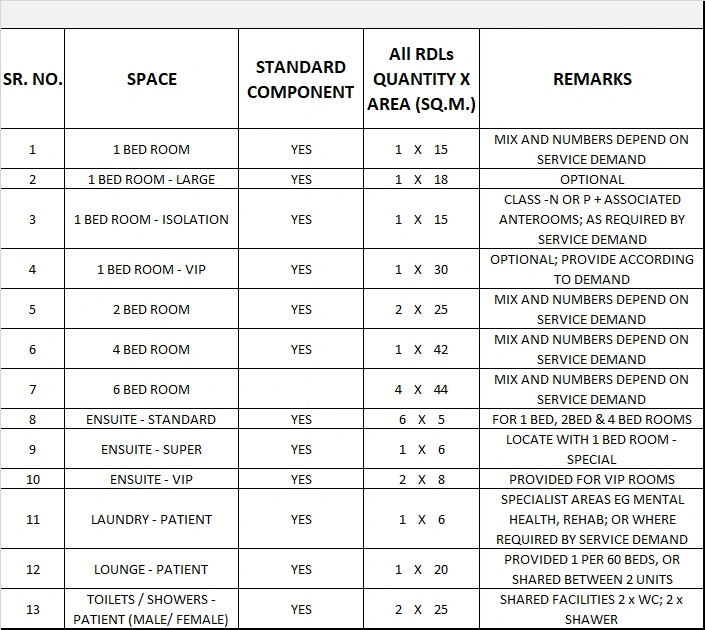
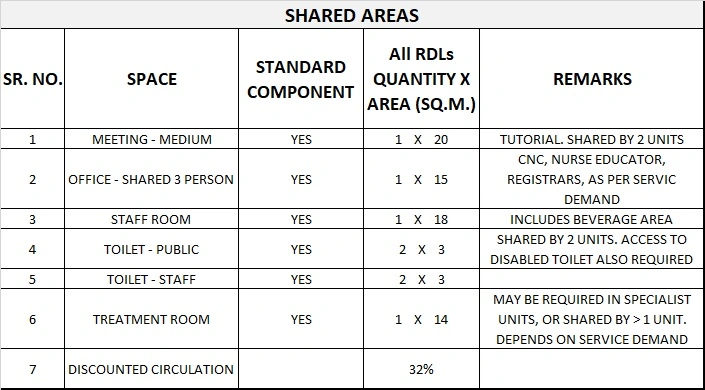
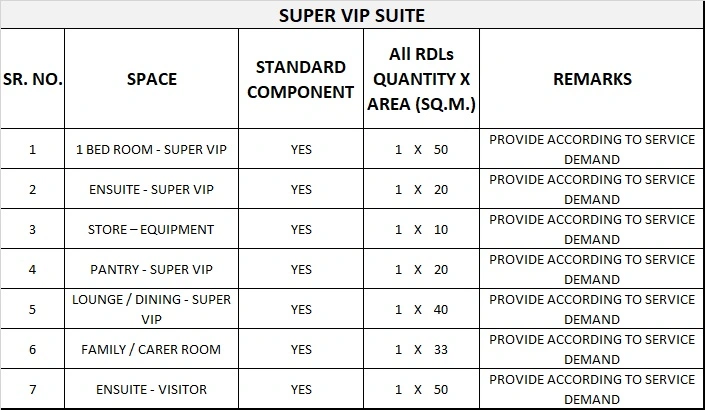
5) Schedule of Accommodation
Inpatient Accommodation Unit Generic Schedule of Accommodation
Schedule of Accommodation for a 30 Bed Unit at all RDS Levels follows. Although categorised by level of service, this does not necessarily lead to different physical requirements.
The Schedule of Accommodation lists generic spaces that form an Inpatient Unit. Quantities and sizes of some spaces will need to be determined in response to the service needs of each unit on a case by case basis.

Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
6) Functional Relationship Diagram
Inpatient Accommodation Unit Functional Relationship Diagram