The Intensive Care Unit (ICU) is one of the most critical components of any healthcare facility. Designed to provide specialized care for patients with life-threatening conditions, the ICU must support highly complex medical interventions, continuous monitoring, and rapid response capabilities.
The design of this space plays a pivotal role not only in how care is delivered but also in ensuring the safety, comfort, and well-being of patients, families, and healthcare staff.
A thoughtfully designed ICU improves clinical outcomes by facilitating seamless workflows, reducing infection risks, and enhancing communication among care teams.
In addition, it contributes to a healing environment through noise control, adequate lighting, and family-friendly spaces—each an essential factor in patient recovery and staff satisfaction.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
Intensive Care is a dedicated unit for critically ill patients who require invasive life support, high levels of medical and nursing care and complex treatment.
The intensive care unit provide a concentration of clinical expertise, technological and therapeutic resources which are coordinated to care for the critically ill patient.
2) Planning of Intensive Care Unit
i) Operational Models
The level of Intensive Care available should support the delineated role of the particular hospital. The role of a particular ICU will vary, depending on staffing, facilities and support services as well as the type and number of patients it has to manage.
There are a number of operational models applicable to intensive care units including:
Combined Critical Care
The Combined Critical Care may include a High Dependency Unit, Intensive Care and/or Coronary Care, often located in a rural or regional hospital where flexibility of bed utilisation is important.
This will allow short and medium term intensive care patients to be managed appropriately when required, and at other times, the Unit may be used for the more common cardiology or high dependency patients.
These Units have lower medical and nursing demands, and will usually be staffed on a nurse/patient ratio of significantly less than ‘one to one’.
Combined General Intensive Care
In this model the Intensive Care consists of all patient specialties such as cardiothoracic surgery, orthopaedics, neurosurgery, and general medical patients. These Units will usually have a combination of intensive care and high dependency beds.
This model may be adopted where there are limited numbers of sub-specialty critical patients. The disadvantage of this model is that if the general intensive care is fully occupied, critical sub specialty cases may need to remain in standard inpatient units for treatment.
Hot Floor
The ‘Hot Floor’ model of Intensive Care can be collocated with specialty Intensive Care Units such as cardiothoracic, neurosurgical and general intensive care and may include a high dependency unit.
A comprehensive ‘Hot Floor’ model may include collocation of ICU with Operating Unit, Emergency, CCU and parts or all of Medical Imaging. The Hot Floor model has the principal advantage of collocating services, avoiding duplication and with a single management structure, allows a more efficient medical and nursing overview.
Advantages of the Hot Floor model include:
- enables standardisation of equipment across the Hot Floor avoiding duplication and minimises service costs
- assists practitioners particularly medical and nursing to develop expertise in the specialties
- prevents access blockage to general ICU beds optimising patient throughput
The disadvantages of a Hot Floor involve:
- the management of a large group of nurses and doctors
- infection control risks including cross infection of patients in co-located units
Separate Intensive Care Units
This model covers a range of specialty Intensive Care Units provided as disconnected units in separate locations, with an independent management structure for each unit.
Advantages of this model include:
- may help to avoid bed blockages by allowing different groups to control the Intensive Care resources
- encourages the development of sub-specialty medical and nursing skills
Disadvantages include duplication of management, policies and procedures and physical isolation of units that may make staffing more difficult.
ii) Functional Areas
The Intensive Care Unit will consist of the following Functional Areas:
- Reception/ Waiting Areas
- Patient Treatment Areas including patient beds, ensuites and treatment rooms
- Support Areas including Utility Rooms, Store Rooms, Linen, Disposal Room, Cleaner’s Room, Pantry
- Administrative / Office Areas
- Staff Amenities Areas.
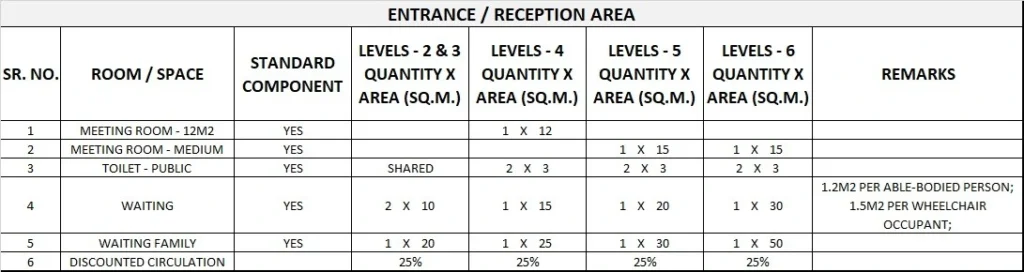
Entry / Reception / Waiting areas
As determined by the size of the ICU and hospital operating policy, a Reception and visitor’s / relatives’ Waiting Areas shall be provided immediately outside the entry to the ICU, but away from patient and staff traffic areas.
It is desirable that this room has provision for a drink dispenser, radio, television and comfortable seating. An Interview Room and a separate area for distressed relatives should be available.
Biomedical Workshop
Dependent upon the size and intended use of the ICU, a dedicated electronic and pneumatic equipment maintenance service may have to be accommodated within the hospital or a 24 hour on-call emergency service made available. This same service would cover the Operating, Emergency and Medical Imaging Units.
If a dedicated workshop is provided, its location should be in an area that is equally accessible to all of the above mentioned departments. The facility should have a degree of soundproofing and be accessible from a non-sterile area.
Laboratory Facilities
All ICUs must have available 24-hr clinical laboratory services. When this service cannot be provided by the central hospital Laboratory, a satellite laboratory within or immediately adjacent to, the ICU must serve this function.
Satellite facilities must be able to provide minimum chemistry and haematology testing, including arterial blood gas analysis.
Overnight Accommodation
Depending upon the availability of nearby commercial accommodation, consideration should be given to the provision of overnight accommodation for relatives and staff, preferably near the unit.
This will be dependent upon the size and intended function of the ICU. A motel type bed-sitter level of provision is recommended.
Special Procedures Room
A Special Procedures Room shall be provided if required by the Operational Policy. If a special Procedures Room is required, it should be located within, or immediately adjacent to, the ICU.
One special Procedures Room may serve several ICUs in close proximity. Consideration should be given to ease of access for patients transported from areas outside the ICU.
Room size should be sufficient to accommodate the necessary equipment and personnel. Monitoring capabilities, equipment, support services, and safety considerations must be consistent with those services provided in the ICU proper.
Work surfaces and storage areas must be adequate enough to maintain all necessary supplies and permit the performance of all desired procedures without the need for staff to leave the room.
Staff Facilities
A Staff Lounge shall be provided within the unit for staff to relax and prepare beverages. Inclusion of a window to the outside is desirable.
A Library/ Reference area with an appropriate range of bench manuals, textbooks and journals for rapid access 24 hours a day should be available within the Intensive Care Unit.
Storage Areas
Mobile equipment such as cardiopulmonary resuscitation trolleys and mobile X-ray, that are used and located within the ICU, shall have storage areas that are out of traffic paths but conveniently located for easy access by staff. Consideration should be given to the ever increasing amount of equipment used in the unit.
iii) Functional Relationships
The ICU should be a separate unit within the hospital with easy access to the Emergency Unit, Operating Unit and Medical Imaging. The location shall be arranged to eliminate the need for through traffic.
3) Design of Intensive Care Unit
i) Patient Treatment Areas
Patients must be situated so that healthcare providers have direct or indirect visualization, such as by video monitoring, at all times.
This approach permits the monitoring of patient status under both routine and emergency circumstances. The preferred design is to allow a direct line of vision between the patient and the central Staff Station.
In ICUs with a modular design, patients should be visible from their respective nursing substations. Sliding glass doors and partitions facilitate this arrangement and increase access to the room in emergency situations
Bedside Monitoring
Bedside monitoring equipment should be located to permit easy access and viewing, and should not interfere with the visualisation of, or access to the patient.
The bedside nurse and/or monitor technician must be able to observe the monitored status of each patient at a glance. This goal can be achieved either by a central monitoring station, or by bedside monitors that permit the observation of more than one patient simultaneously.
Neither of these methods are intended to replace bedside observation. Weight-bearing surfaces that support the monitoring equipment should be sturdy enough to withstand high levels of strain over time.
It should be assumed that monitoring equipment will increase in volume over time. Therefore, space and electrical facilities should be designed accordingly.
ii) Environmental Considerations
Acoustics
Signals from patient call systems, alarms from monitoring equipment, and telephones add to the sensory overload in critical care units. Without reducing their importance or sense of urgency, such signals should be modulated to a level that will alert staff members, yet be rendered less intrusive.
For these reasons, floor coverings that absorb sound should be used while keeping infection control, maintenance, and equipment movement needs under consideration. Walls and ceilings should be constructed of materials with high sound absorption capabilities.
Ceiling soffits and baffles help reduce echoed sounds. Doorways should be offset, rather than being placed in symmetrically opposed positions, to reduce sound transmission.
Counters, partitions, and glass doors are also effective in reducing noise levels. Please refer to () “Acoustic Solutions for Healthcare Facilities”
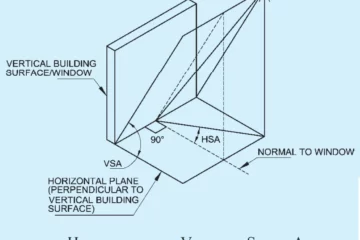
Natural Light
Natural light and views should be available from the Unit for the benefit of staff and patients. Windows are an important aspect of sensory orientation, and as many rooms as possible should have windows to reinforce day/ night orientation.
If windows cannot be provided in each room, an alternate option is to allow a remote view of an outside window or skylight.
iii) Space Standards And Components
Where an open plan arrangement is provided, bed spaces shall be arranged so that there is a clearance of at least 1200 mm from the side of the bed to the nearest fixed obstruction (including bed screens) or wall.
At the head of the bed, at least 900 mm clearance shall be allowed between the bed and any fixed obstruction or wall.
When an open plan arrangement is provided, a circulation space of 2200 mm minimum clear width shall be provided beyond dedicated cubicle space.
Separate cubicles and Single Patient Bedrooms including Isolation Rooms, shall have minimum dimensions of 3900 mm x 3900 mm.
iv) Finishes
In all areas where patient observation is critical, colours shall be chosen that do not alter the observer’s perception of skin colour.
v) Fixtures & Fittings
Clocks
An analogue clock/s with a second sweep hand shall be provided and conveniently located for easy reference from all bed positions and the Staff Station.
Bedside Storage
Each patient bed space shall include storage and writing provision for staff use.
Window Treatments
Window treatments should be durable and easy to clean. Consideration may be given to use of double glazing with integral blinds, tinted glass, reflective glass, exterior overhangs or louvers to control the level of lighting.
vi) Infection Control
Handbasins
Clinical Hand-washing Facilities shall be provided convenient to the Staff Station and patient bed areas. The ratio of provision shall be one clinical hand-washing facility for every two patient beds in open-plan areas and one in each patient Bedroom or cubicle.
Isolation Rooms
At least one negative pressure Isolation Room per ICU shall be provided in Level 5 and 6 facilities. Entry shall be through an airlock.
Clinical hand-washing, gown and mask storage, and waste disposal shall be provided within the airlock. An Ensuite – Special, directly accessible from the Isolation Room, shall also be provided.
All entry points, doors or openings, shall be a minimum of 1200 mm wide, unobstructed. Larger openings may be required for special equipment, as determined by the Operational Policy.
vii) Building Service Requirements
Mechanical Services
The unit shall have appropriate air conditioning that allows control of temperature, humidity and air change. Refer to Part E of these Guidelines for the specific requirements for Mechanical and Electrical provision.
Communications
All ICUs should have an intercommunication system that provides voice linkage between the Staff Station, Patient Modules, Staff-Overnight Stay Rooms, Conference Rooms, and Staff Lounge.
Supply Areas and the Visitors’ Lounge / Waiting Room may also be included in the system. When appropriate, linkage to key departments such as Blood Bank, Pharmacy, and Clinical Laboratories should be included.
In addition to a standard telephone service for each ICU, which should provide hospital-wide and external communications capabilities, there should be a mechanism for emergency internal and external communications when normal systems fail.
4) Components of the unit
i) Standard Components
The Intensive Care Unit will consist of Standard Components to comply with details in Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets
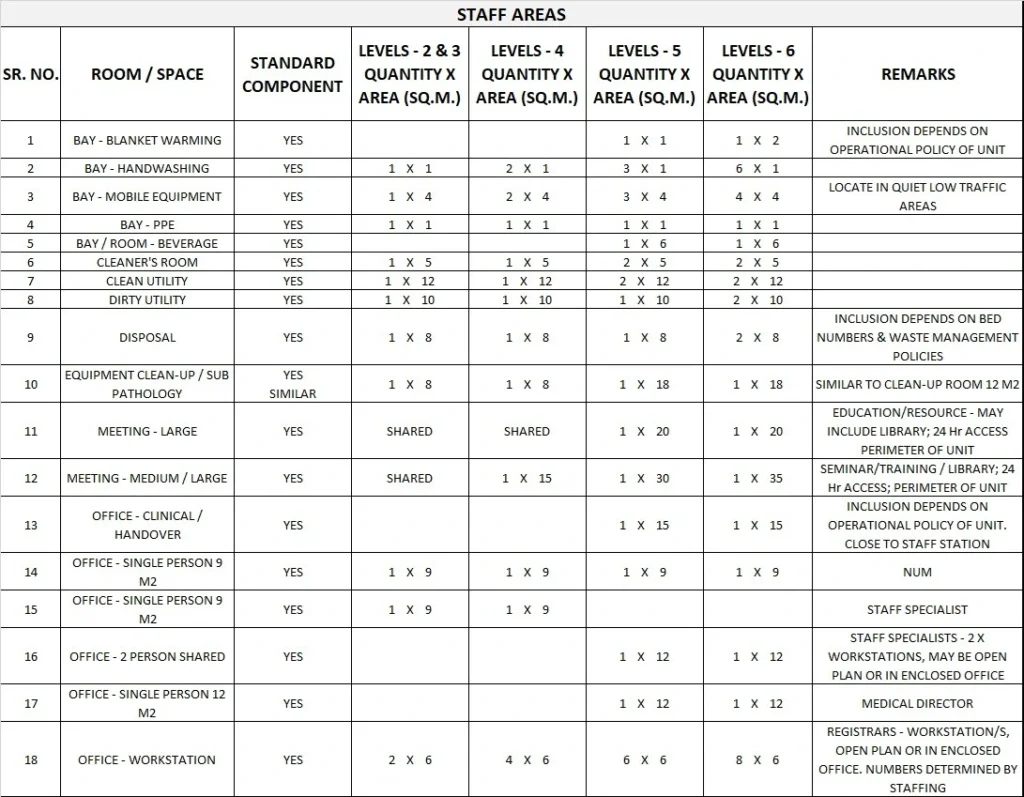
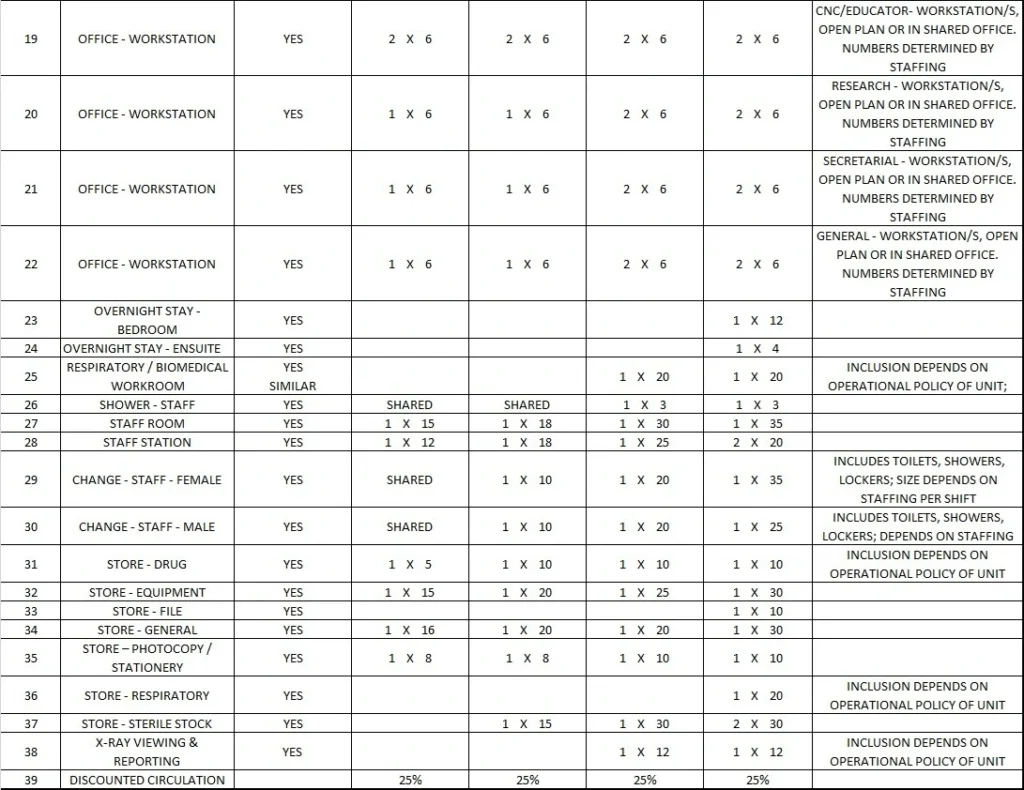
5) Schedule of Accommodation
Intensive Care Unit Generic Schedule of Accommodation
Schedule of Accommodation for Units at Levels 3, 4, 5, and 6 follows.
The Schedule of Accommodation lists generic spaces that form an Intensive Care Unit. Quantities and sizes of some spaces will need to be determined in response to the service needs of each unit on a case by case basis.
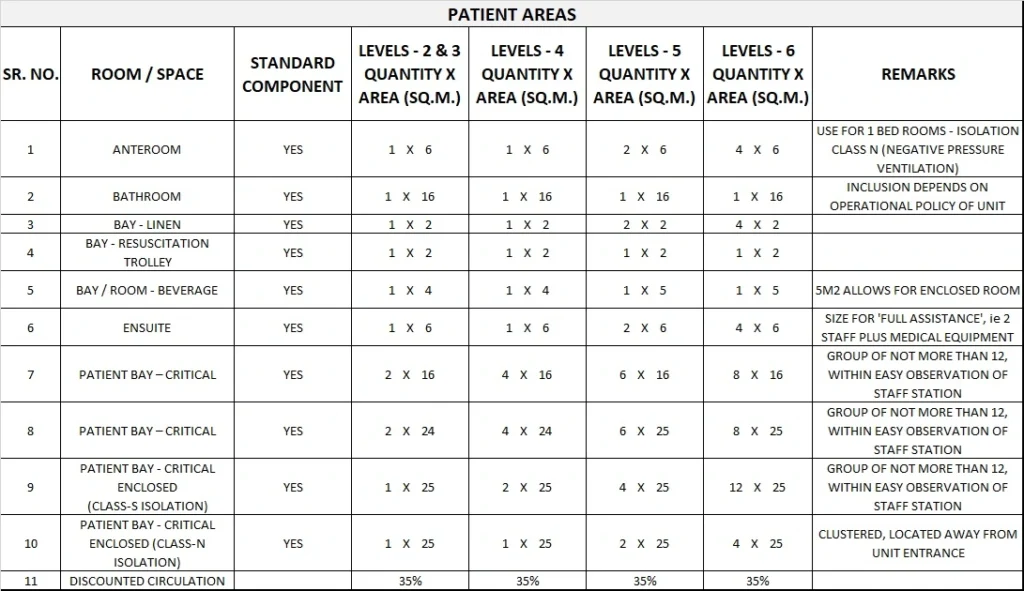
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
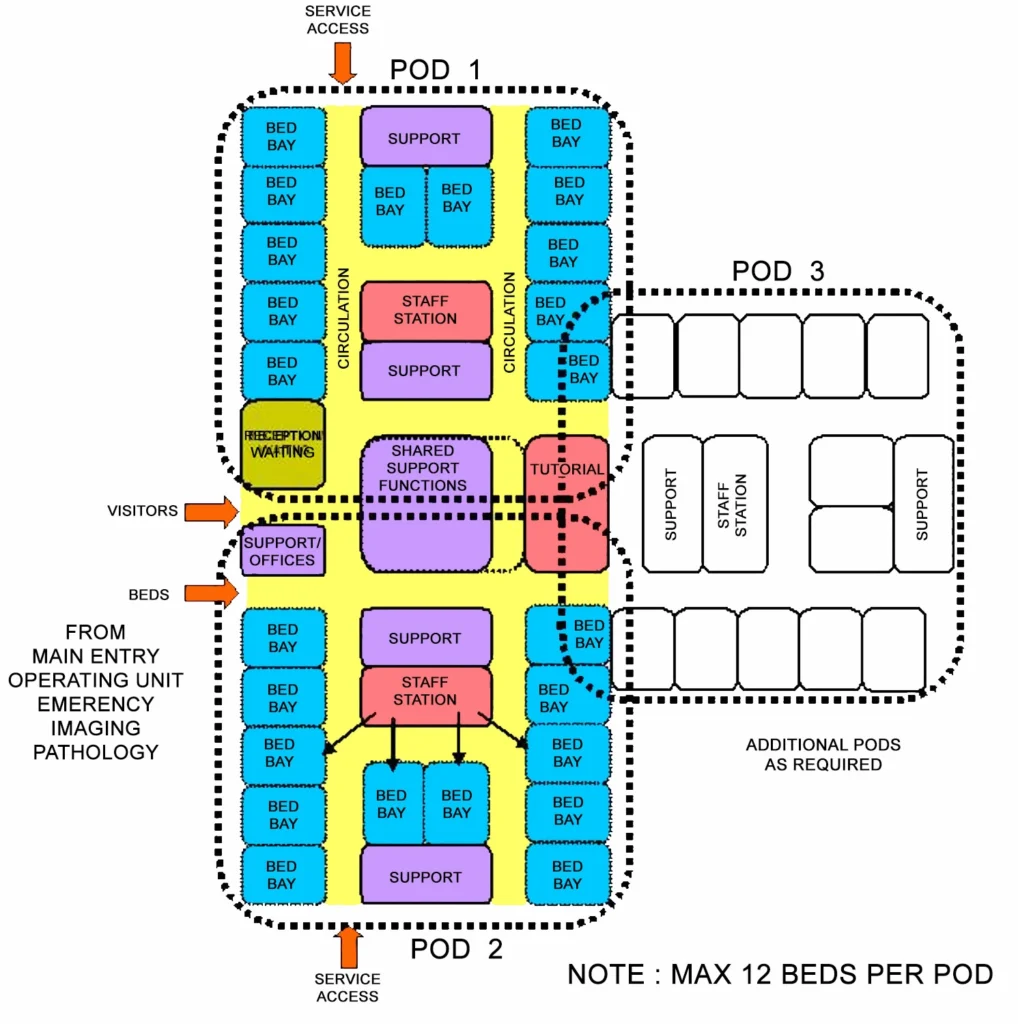
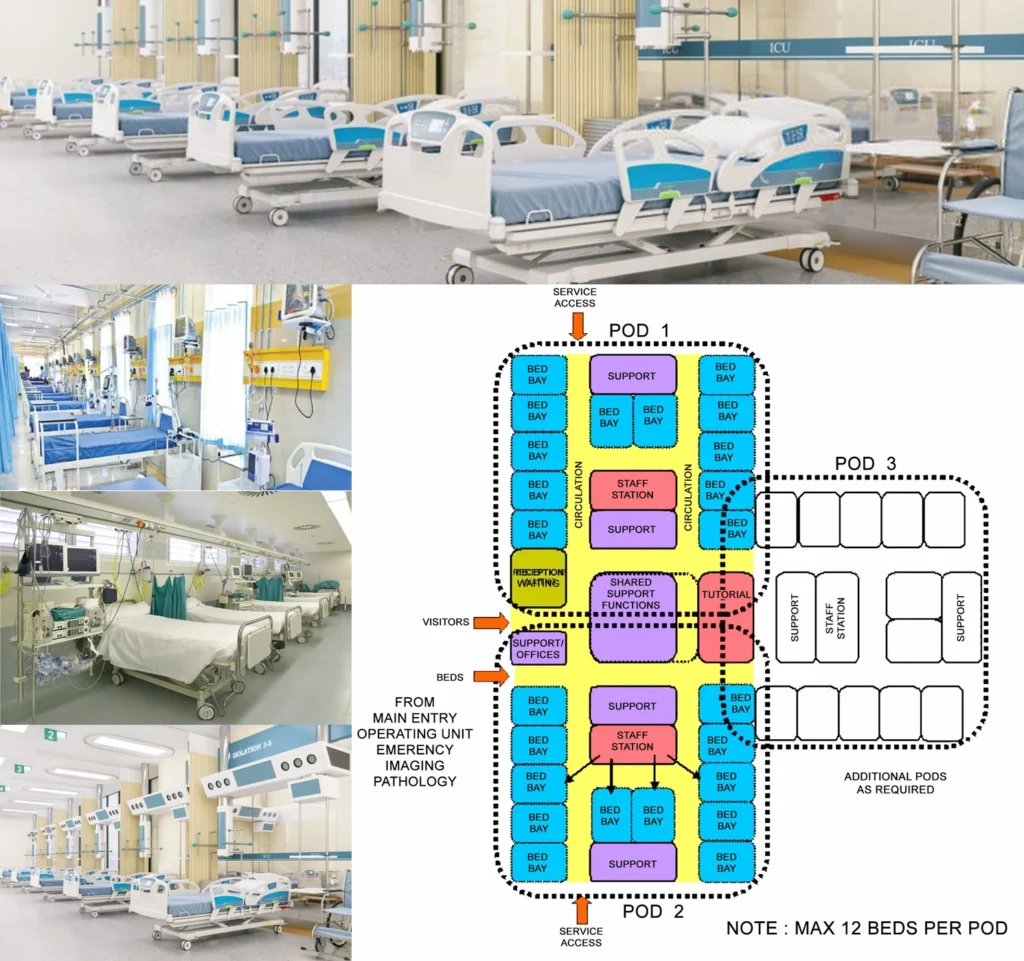
6) Functional Relationship Diagram
Intensive Care Unit Functional Relationship Diagram