A well-designed emergency unit is the backbone of any healthcare facility, ensuring that patients receive timely, efficient, and high-quality care during critical moments. Proper design directly impacts workflow, patient safety, and overall medical outcomes.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Description
The function of the Emergency Unit is to receive, stabilise and manage patients (adults and children) who present with a large variety of urgent and non urgent conditions whether self or otherwise referred.
The Emergency Unit also provides for the reception and management of disaster patients as part of the Unit’s role within each region.
It is recommended that Hospitals that do not provide an Emergency Service display a prominent exterior sign at the main entrance stating this and giving the location of the nearest Hospital with an Emergency Service.
2) Planning of Emergency Unit
Operational Models
The Emergency Unit may be configured in a number of models that may influence facility design including
i) Fast-Track
Specific patient groups may be assessed and treated via a separate ‘fast’ track to other EU presentations. This may occur at the triage point, or immediately after triage but in a separate zone.
Patient types suitable for this area may include contagious diseases, minor injuries, ambulatory paediatrics. Assessment and treatment may be carried out in Consult / Examination rooms.
ii) Grouping by patient acuity
Patients of similar acuity (urgency) or staff intensity may be treated in the same zone. Facilities for this model will include separate areas for resuscitation, acute monitored beds, acute non monitored beds and ambulatory treatment spaces.
There may be separate entrypoints (or triage points) for the different areas. Staff may be separately allocated to different areas for each shift, and may require separate Staff Stations and private workspace.
iii) Grouping by specialty
Patients may be managed in different areas according to the specialty of service they require e.g. acute treatment, complex investigation, complex discharge planning, or paediatrics.
Patients may be triaged from a central arrival point, or from separate ambulance and ambulant entry points. Within each Functional Area, patients would be prioritised according to acuity.
In this model, separate staffing for each area is required, which would also include separate workspaces for staff.
iv) Other special functions
Short Stay Wards /Emergency Medicine Unit/ Observation Units may be located adjacent or incorporated into the Emergency Unit. This may allow sharing of administrative, staff and support facilities.
Functional Areas
An Emergency Unit may include the following Functional Areas:
i) Entrance / Reception / Triage
- Receiving of patients and visitors and administration
- Assessment for patients
ii) Patient Treatment areas
- Assessment and treatment areas including Resuscitation, Acute Treatment bays/ rooms, Seclusion Room and Decontamination Facility, Paediatric patient areas, Procedure Rooms
- Short-Stay Ward/ Emergency Medicine Unit/ Observation Unit;
- Primary Care Area – for patients with low acuity conditions;
- Stepdown Area – for patients awaiting test results, considered safe, but requiring observation prior to admission or discharge.
iii) Staff and Support areas
- Clean and Dirty Utility Rooms
- Store rooms
- Linen
- Waste Holding/ Cleaners rooms
- Staff amenities, administrative and teaching functions;
- Ambulance facilities.
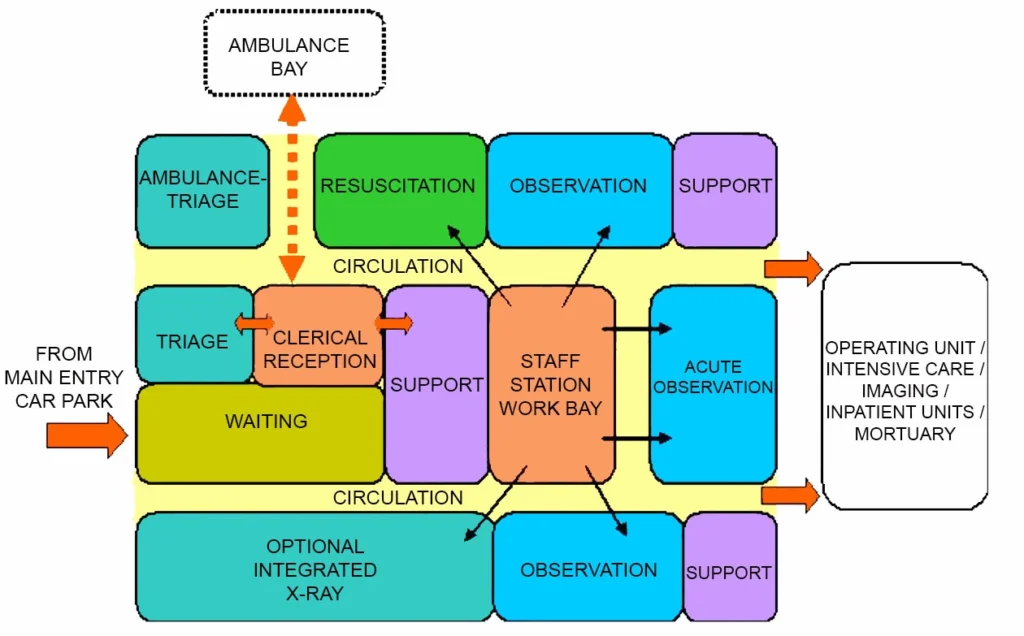
The main aggregation of clinical staff will be at the Staff Station in the Acute Treatment / Resuscitation Area. This should be the focus around which the other clinical areas are grouped. The Entrance/Reception Area is the focus of initial presentation.
- In addition to standard treatment areas, some departments may require additional, specifically designed areas to fulfil special roles, such as:
- Management of paediatric patients
- Management of major trauma patients
- Management of psychiatric patients
- Management of patients following sexual assault
- Extended observation and management of patients
- Undergraduate and postgraduate teaching
- Transport and retrieval services
- Telemedical referral/ consultation service
iv) Entrance area
The entrance to the Emergency Unit must be at grade-level, well-marked, illuminated, and covered. It shall provide direct access from public roads for ambulance and vehicle traffic, with the entrance and driveway clearly marked. A ramp shall be provided for pedestrian and wheelchair access.
The entrance to the Emergency Unit shall be paved to allow discharge of patients from cars and ambulances. Temporary parking should be provided close to the entrance.
v) Waiting area
The Waiting Area should provide sufficient space for waiting patients as well as relatives / escorts. The area should be open and easily observed from the Triage and Reception areas. Seating should be comfortable and adequate.
Space should be allowed for wheelchairs, prams, walking aids and patients being assisted. There should be an area where children may play. Support facilities, such as a television should also be available.
Fittings must not provide the opportunity for self harm or harm towards staff. Waiting Areas shall be negatively pressured. From the Waiting Area there must be access to:
- Triage and Reception Areas
- Toilets
- Baby Change Room
- Light refreshment facilities which may include automatic beverage dispensing machines
- Telephone and change machines
- Health literature
It is desirable to have a separate Waiting Areas particularly for children. Child play areas will provide equipment suitable for safe play activities, including a television.
It shall be separated for sound from the general Waiting Rooms and must be visible to the Triage Nurse. The area should be monitored to safeguard security and patient well being.
vi) Reception / Clerical areas
The Reception Area is required to accommodate:
- Reception of patients and visitors
- Registration interviews of patients
- Collation of clinical records
- Printing of identification labels.
The counter should provide seating and be partitioned for privacy at the interview area. There should be direct communication with the Reception / Triage area and the Staff Station in the Acute Treatment / Observation Area.
The Reception/Clerical Area should be designed with due consideration for the safety of staff. This area requires a duress alarm.
vii) Reception / Triage
The Reception / Triage and Staff Station shall be located where staff can observe and control access to treatment areas, pedestrian and ambulance entrances, and public waiting areas. This area requires a duress alarm.
The Emergency Unit should be accessible by two separate entrances: one for ambulance patients and the other for ambulant patients. It is recommended that each entrance area contains a separate foyer that can be sealed by remotely activating the security doors.
Access to Treatment Areas should also be restricted by the use of security doors. The Ambulance Entrance should be screened as much as possible for sight and sound from the ambulant patient entrance. Both entrances should direct patient flow towards the Reception/Triage Area.
The Reception / Triage area should have clear a vision to the Waiting Room, the children’s play area (if provided) and the ambulance entrance. The Reception / Triage Area may perform observations and provide first aid in relative privacy.
viii) Acute Psychiatric Emergency Care Area
The patient who is suffering from an acute psychological or psychiatric crisis has unique and often complex requirements. An Emergency Unit should have adequate facilities for the reception, assessment, stabilisation and initial treatment of patients presenting with acute mental health problems.
It is not intended that this be used for prolonged observation of uncontrolled patients. The main purpose of such an area is to provide a safe and appropriate space to interview and stabilise patients.
Acute mental health presentations have the potential to disrupt the normal operation of an Emergency Unit. Conversely, the busy environment of an Emergency Unit may not be conductive to the care of patients with acute mental health crises.
Patient flows should be separated where possible to maximise privacy and minimise disruption. A separate secure entrance for use by community emergency mental health teams and police may be desirable. Patients should be continuously observable by staff either directly or via closed circuit television
The designated area should be within close proximity of other continuously staffed areas of the department, with ready access to assistance when required, As far as possible, the facility should not contain objects that could be thrown at staff. There should be two separate exits to allow the exit of staff if one exit is blocked.
The exit doors should open outwards, and should be lockable from the outside but not from the inside. If a window is incorporated, any drapes or blinds shading the window should be operable from outside. All areas should have easily accessible duress alarms.
As far as possible, the area should be free of heavy or breakable furniture, sharp or hard surfaces which could injure an uncontrolled patient, and should incorporate tamper resistant electrical fittings.
It should also incorporate interior design features that promote calmness, such as muted colours and soft furnishings and appropriate lighting. Patient tracking devices may enhance security.
The Acute Psychiatric Emergency Care Area should be separate enough from adjacent patient care areas to allow privacy for the mental health patient and protection of other patients from potential disturbance or violence.
There should be acoustic and visual separation from adjacent clinical areas, but ready access for staff in the event of an urgent need for intervention. The incorporation of sound-insulating material is recommended.
Please refer to Part C, 9.2 “Acoustic Solutions for Healthcare Facilities” Ideally the Acute Psychiatric Emergency Care Area facility should contain at least two separate but adjacent areas:
Interview Room (Mental Health)
This room should have two exit doors, swinging outward and lockable from outside, to allow for the escape of staff members when one exit is blocked. One door should be large enough to allow a patient to be carried through it. Consideration should be given to installing a solid door with safety viewing glass.
The Interview Room should also be:
- Shielded from external noise
- Furnished with only soft furnishings with no hard edges
- Designed in such a way that observation of the patient by staff outside the room is possible at all times; this may be backed up with closed circuit television for the safety of staff
- Arranged to ensure that patients have no access to air vents or hanging points
- Fitted with a smoke detector
- Fitted with duress alarm at each exit.
Examination / Treatment room (Mental Health)
The Examination/Treatment Room should be immediately adjacent to the Interview room. It should contain adequate facilities for physical examination of the patient, however the inclusion of unnecessary and easily dislodged equipment should be avoided.
If operational policy dictates that intravenous sedation is to occur in this area, it should contain the appropriate facilities and monitoring equipment, mounted out of reach of a potentially violent patient. It should contain the minimum of additional fittings or hard furnishings that could used to harm an uncontrolled patient.
It should be of sufficient size to allow a restraint team of five people to surround a patient on a standard Emergency Unit bed and should be at least 12 m2 in floor area.
ix) Acute Treatment Areas
Acute Treatment Areas are used for the management of patients with acute illnesses. Requirements are as follows:
- Areas to fit a standard mobile bed
- Storage space for essential equipment
- Space to allow monitoring equipment to be housed
- Minimum space between beds is 2.4 m
- Each treatment area must be at least nine m2 in area
All Treatment Areas, including Triage, require the following:
- Service panel
- Examination light; the examination light must be a high standard focused light with a power output of 30,000 lux, illuminate a field size of least 150 mm and be of robust construction
- Wall mounted sphygmomanometer
- Shelving
- Waste bins and sharps containers
- Patient call and emergency call facilities
x) Patient toilets / Showers
In an Emergency Unit the following Patient Toilet / Ensuite facilities will be required, (separate Male and Female):
- Up to eight treatment bays – two Patient Toilets / Ensuite, one each for male / female
- Between nine and 20 treatment bays – four Patient Toilets / Ensuite, two each for male / female
- Between 21 and 40 treatment bays – six Patient Toilet / Ensuite, three each for male / female
- More than 40 treatment bays – eight Patient Toilet / Ensuite, four each for male / female
- At least two of the above Toilets / Ensuites to be Accessible for wheelchairs, one each for male / female.
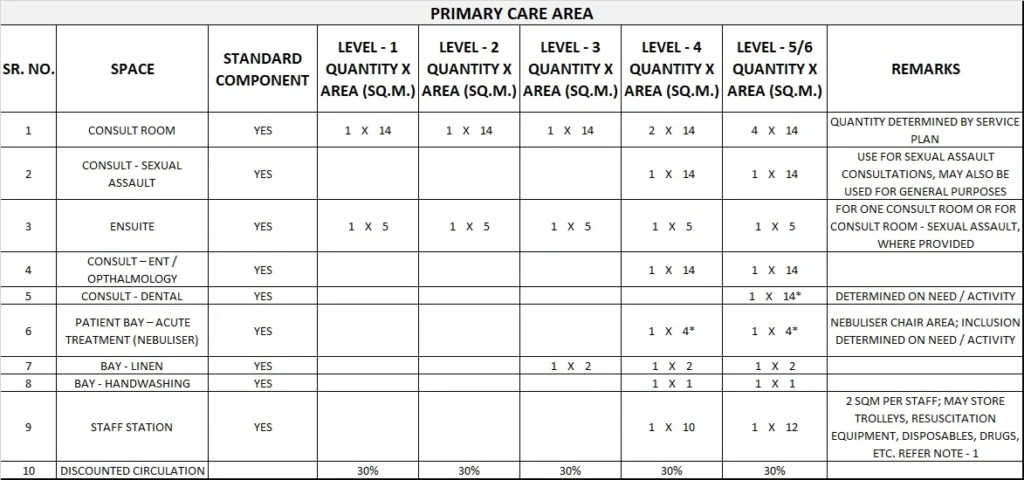
xi) Consultation Areas
Consultation Room/s are to be provided according to Unit size and requirements for examination and treatment of ambulant patients. Consult Rooms are to comply with Standard Components – Consult Room.
xii) Consultation – Outpatients
If an Outpatient Consultation Service is to be provided according to the service plan, the following facilities shall be provided:
- Entrance and Reception; this may be a shared facility with the hospital or other specialty departments
- Waiting Area may be shared
- Consulting / Examination room/s
- Treatment Room/s
- Nurses Office; dependent upon the size of the outpatient service
- Medical Laboratory / Utility Room; the size and type of this facility will be determined by the size of the outpatient service and whether or not shared facilities are available within the hospital
- Dirty Utility / Disposal Room
- Staff Room; may be shared with the hospital
- Toilets and Change Rooms; may be shared with the hospital
- Storage; as required
- Cleaner’s Room; may be shared with the hospital
- Environmental Requirements; special attention is to be given to the visual and acoustic privacy of patients when being interviewed and also to the quality of light when being examined (the latter requires adequate natural light or colour corrected artificial lighting or task lighting)
- Miscellaneous: construction, finishes, design for disabled access, parking, signposting etc., shall be in accordance with the other relevant sections of these Guidelines.
xiii) Decontamination Area
An Isolation Room should be available for patients who are contaminated with toxic substances. In addition to the requirements of an Isolation Room, this room must:
- Be directly accessible from the ambulance bay without entering any other part of the unit
- Have a flexible water hose, floor drain and contaminated water trap.
xiv) Laboratory Area
A designated area for performing laboratory investigations such as arterial blood gas analysis and microscopy should be considered in Units of Levels 5 or 6.
xv) Pharmacy / Medication Area
A Pharmacy / Medication area is required for the storage of medications used within the Emergency Department. Entry should be secure with a self-closing door.
The area should be accessible to all clinical areas and have sufficient space to house a refrigerator, which is essential for the storage of heat sensitive drugs.
xvi) Resuscitation Area
The Resuscitation Room/ Bay is used for the resuscitation and treatment of critically ill or injured patients. The Resuscitation Room/ Bay requires:
- Space to fit a specialised resuscitation bed
- Space to ensure 360 degree access to all parts of the patient for uninterrupted procedures
- Circulation space to allow movement of staff and equipment around the work area
- Space for equipment, monitors, storage, wash up and disposal facilities
- Appropriate lighting and equipment to hang IV fluids
- Maximum possible visual and auditory privacy for the occupants of the room and other patients and relatives
- Easy access from the ambulance entrance and separate from patient circulation areas
- Easy access to the Acute Treatment/Observation area from the Staff Station
- A full range of physiological monitoring and resuscitation equipment
- Workbenches, storage cupboards, handbasins, X-ray viewing facilities (or digital electronic imaging system) and computer access
- Solid partitions between this and other areas are recommended.
Each Resuscitation Bay should be equipped with:
- Service panel, service pendants or pods to maximise access to patients
- Physiological monitor with facility for ECG, printing, NIBP, SpO2, temperature probe, invasive pressure, C02 monitor
- A light similar to a small, single arm operating light
- Resuscitation patient trolley
- Wall mounted diagnostic set (ophthalmoscope/ auroscope)
- Overhead IV track
Imaging facilities should include:
- Overhead X-ray
- X-ray screening (lead lining) of walls and partitions between beds
- Resuscitation trolley with X-ray capacity
xvii) Staff Station
The Staff Station should have an uninterrupted vision of the patients. It should be centrally located and be constructed as an enclosed area to ensure confidential information can be conveyed without breach of privacy and to provide security to staff, information and privacy.
The use of sliding windows and adjustable blinds can be used to modulate external stimuli and a separate write-up area may be considered.
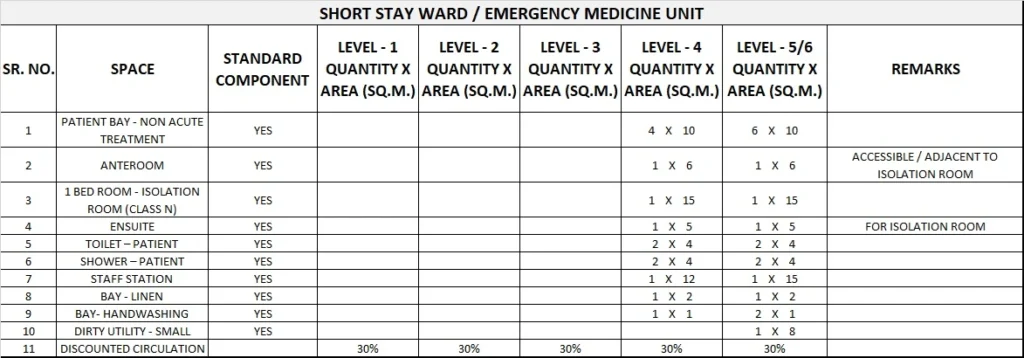
xviii) Short stay ward / Emergency Medical Unit (EMU)
This facility may be provided either within or adjacent to the Emergency Unit for the prolonged observation and ongoing treatment of patients who are planned for subsequent discharge (directly from the EU). Patients may be kept in this Unit for diagnosis, treatment, testing or for medical stabilisation.
The length of stay in the Unit is generally between 4 and 24 hours, although Unit policy may require longer stays. The Unit may also be situated separately to the Emergency Unit, although functionally linked.
According to the service plan, dedicated beds for short stay are separately designated and staffed. The types of patients planned to be admitted to this Unit will determine the number and type of beds provided, and the design of associated monitoring and equipment. Staff Stations, work and storage and other support areas will need to be available and may be
shared if the unit is located physically close to other treatment areas.
Functional Relationships
The design should allow for rapid access to every space with a minimum of cross traffic. There must be close proximity between the Resuscitation / Acute Treatment areas for non-ambulant patients, other treatment areas for non-ambulant patients and other treatment areas for ambulant patients, so that staff may be relocated at times of high workload.
Visitor and patient access to all areas should not traverse clinical areas. Protection of visual, auditory and olfactory privacy is important whilst recognising the need for observation of patients by staff.
The Emergency Unit will require ready access to the following key functional areas:
- Medical Imaging Unit
- Operating Unit – rapid access is highly desirable for surgical emergencies
- Coronary Care Unit
- Pathology / Blood Bank Unit
- Clinical Records Unit
- Inpatient Accommodation Unit
- Pharmacy Unit – proximity is required
- Outpatients (if an outpatient service is provided adjacent to the Emergency Unit)
- Mortuary
i) Clinical Records
Access to clinical records is required so that patients’ previous medical histories are obtainable without delay. A system of mechanical or electronic clinical record transfer is desirable to minimise delays and labour costs. Access to clinical records must be available 24 hours per day.
ii) Medical Imaging
The Medical Imaging Unit should have a general X-ray table and upright X-ray facilities. It is possible to provide Medical Imaging as a satellite facility within the Emergency Unit.
Additionally, an overhead gantry in the resuscitation area may be provided. The presence/ absence of a film processor is dependent upon close proximity to the main Medical Imaging Department or the use of digital radiology.
Immediate access to CT scanning, Ultrasound and Nuclear Medicine modalities will enhance the Emergency Unit’s effectiveness. A system of electronic display of imaging is desirable.
iii) Pathology
Rapid access to Pathology services is highly desirable to minimise turnaround times for laboratory investigations. Mechanical or pneumatic tube transport systems for specimen and electronic reporting of results are recommended. Point of care access for electrolyte and blood gas analysis is highly desirable.
iv) Pharmacy
Proximity to the Pharmacy Unit is desirable to enable prescriptions to be filled by patients with limited mobility.
2) Design of Emergency Unit
i) Location and Design
Decisions regarding the site location have a major influence on the eventual cost and operational efficiency of the Emergency Unit staff.
The site of the Emergency Unit should, as much as possible, maximise the choices of layout. In particular, sites of access points must be carefully considered.
The Emergency Unit should be located on the ground floor for easy access. It should be adequately signposted
ii) Car Parking
Car parking should be close to the Entrance, well lit and available exclusively for patients, their relatives and staff. Parking areas should be available close to the Emergency Unit for urgent call in staff.
Undercover car parking should be available for:
- Appropriate number of ambulances which will be determined by the case load and the availability of ambulance access to other parts of the hospital for non emergency patients
- Taxis and private vehicles that drop off/pick up patients adjacent to the ambulance entrance.
iii) Signage
The emergency unit should be clearly identified from all approaches. Signposting that is illuminated is desirable to allow visibility at night. The use of graphic and character displays such as a white cross on a red background is encouraged.
iv) Environmental Considerations
Acoustics
Clinical Areas should be designed to minimise the transmission of sound between adjacent treatment areas. The following areas will require acoustic consideration:
- Consult/ Interview and triage areas for discussions / interviews with clients;
- Seclusion and psychiatric assessment rooms
- Treatment and Procedure Rooms;
- Waiting areas
- Staff Stations
Natural light
The use of natural light should be maximised throughout the Unit. Natural lighting contributes to a sense of wellbeing and assists orientation of patients and visitors and minimises staff disorientation.
v) Infection Control
Handbasins for hand-washing should be available within each treatment area and should be accessible without traversing any other clinical area.
All handbasins in clinical areas should be of surgical type with hands-free activation (Type A). Dispensers for non sterile latex gloves should be available in the vicinity of each handbasin and each treatment area. Refer to Part D- Infection Control for ratios of basins required in clinical areas.
vi) Isolation Rooms
At least one negative pressure Isolation Room should be provided in Units in Level 5 & 6. The need for additional negative pressure Isolation Rooms shall be determined by the infection control risk assessment. Refer to Infection Control Part D.
vii) Space Standards and Components
Bed Spacing
In the Acute Treatment Area there should be at least 2.4 metres of clear floor space between beds. The minimum length should be three metres.
Corridors
In general, the total corridor area within the department should be minimised to optimise the use of space. Where corridors are necessary, they should be of adequate width to allow the cross passage of two hospital beds without difficulty.
There should be adequate space for trolleys to enter or exit any of the Consulting Rooms, and to be turned around. Standard corridors should not be used for storage of equipment.
Note: Refer to Part C – Space Standards & Dimensions for corridor standards.
viii) Safety and Security
The Emergency Unit receives a large number of patients and their visitors, many of whom may be distressed, intoxicated or involved in violence.
The hospital has a duty of care to provide for the safety and security of employees, patients and visitors. Both policies and structures should be in place to minimise injury, psychological trauma and damage or loss of property.
The precise details of security features should be designed in conjunction with a security risk assessment for the specific site.
The location of an office for security personnel near the entrance should be considered. This room should be positioned so that it allows Security Staff a clear view of the Waiting Room, Triage and Reception Areas.
Immediate access to these areas is essential. Remote monitoring of other areas in the department by CCTV and of staff duress/personal alarms should also occur from this area.
Perimeter Access Control
Ambulatory and Ambulance entrances should be separate, with electronically operated locks. Access from the Waiting Areas to the treatment areas should be controlled.
There should be restricted access from the remainder of the hospital into the Emergency Unit.
Reception / Triage Areas
The interface between the Waiting Areas and the Reception / Triage Areas should be carefully designed so as to permit communication and reassurance to distressed patients or visitors, yet provide safety and security for staff.
Counters should be of sufficient height and depth to minimise the possibility of them being jumped over or reached over.
The Reception Area should be elevated so that staff may sit at eye level with standing patients or visitors. The Reception / Triage area should have an unobstructed view of the entire Waiting Area.
Fixed and/or personal duress alarms should be positioned in suitable areas as suggested by the security risk assessment. Uniformed security personnel may be required at very short notice to assist with a safety or security issue.
Relatively secluded or isolated areas should be monitored electronically (for example, by closed circuit television), with monitors in easily visible and continuously staffed areas.
ix) Finishes
Wall protection
Hospital beds, ambulance trolleys, and wheelchairs may cause damage to walls. All wall surfaces in areas which may come into contact with mobile equipment should be reinforced and protected with buffer rails or similar.
Floor Finishes
The floor finishes in all patient care areas and corridors should have the following characteristics:
- Non-slip surface
- Impermeable to water, body fluids
- Durable
- Easy to clean
- Acoustic properties that reduce sound transmission. Please refer to Part C, 9.2 “Acoustic Solutions for Healthcare Facilities”
- Shock absorption to optimise staff comfort but facilitate movement of beds Office/s, Tutorial Rooms, Staff Rooms, Clerical Areas and the Distressed Relatives’ Room should be carpeted.
x) Building Service Requirements
Communications
Emergency Units are high volume users of telecommunications and information technology. Telephones should be available in all offices, at all staff stations, in the clerical area and in all consultation and other clinical rooms. The use of multi-function, wireless communication devices should be considered.
Additional phone jacks should be available for the use of facsimile machines and computer modems where required. A dedicated telephone to receive admitting requests from outside medical practitioners is desirable. A cordless phone or phone jack should be available for access to patients’ beds.
An electronic Emergency Unit Information System may be installed to support clinical management, patient tracking and departmental administration. Sufficient terminals should be available to ensure that queuing does not occur, even at peak times.
Workspace design should include sufficient bench-widths or suitable suspension devices for terminals, keyboards, drives and printers. Additional computer terminals, software and peripheral devices should be installed to enable other departmental functions
An intercom or public address system that can reach all areas of the Emergency Unit should be considered. Public telephones with acoustic hoods should be available in the Waiting Area.
A direct line to a taxi company is desirable. Direct telephone lines bypassing the hospital switchboard should be available for use in internal and external emergencies or when the hospital PABX is out of service.
The Staff Station should have a dedicated inward line for the for the ambulance and police services. There should be facsimile lines in clerical areas as well as between the ambulance service and the Emergency Unit, including incoming aeromedical transport.
Nurse Call
All patient spaces and clinical areas, including beds, toilets, bathrooms, treatment areas, patient day areas and lounges should have access to an emergency call facility so staff can summon urgent assistance. The emergency call facility should alert to a central module situated adjacent to the Staff Station, as well as to the Staff and Tutorial rooms.
Telemedicine
Emergency Units using telemedicine facilities should have a dedicated, fully enclosed room with appropriate power and communications cabling provided. This room should be of suitable size to allow simultaneous viewing by members of multiple service teams and should be close to the Staff Station.
3) Components of the Unit
The Emergency Unit will consist of a combination of Standard Components and Non Standard Components. Provide Standard Components to comply with details in Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets.
i) Non Standard Components
Communications Room – Ambulance
Description and Function
The Ambulance Communications Room is occupied by up to three ambulance officers to communicate between major hospital centres and the ambulance service for coordination of Ambulance movements. The communications base is also a critical co-ordination centre in the event of a disaster.
Location and Relationships
The room should be immediately adjacent to the Ambulance entry of the Emergency Unit with direct line of sight to incoming ambulance vehicles and the parking bays.
Considerations
The room will include:
- Workstation benches and chairs for 3 persons
- Telephones, computer and radio communications systems
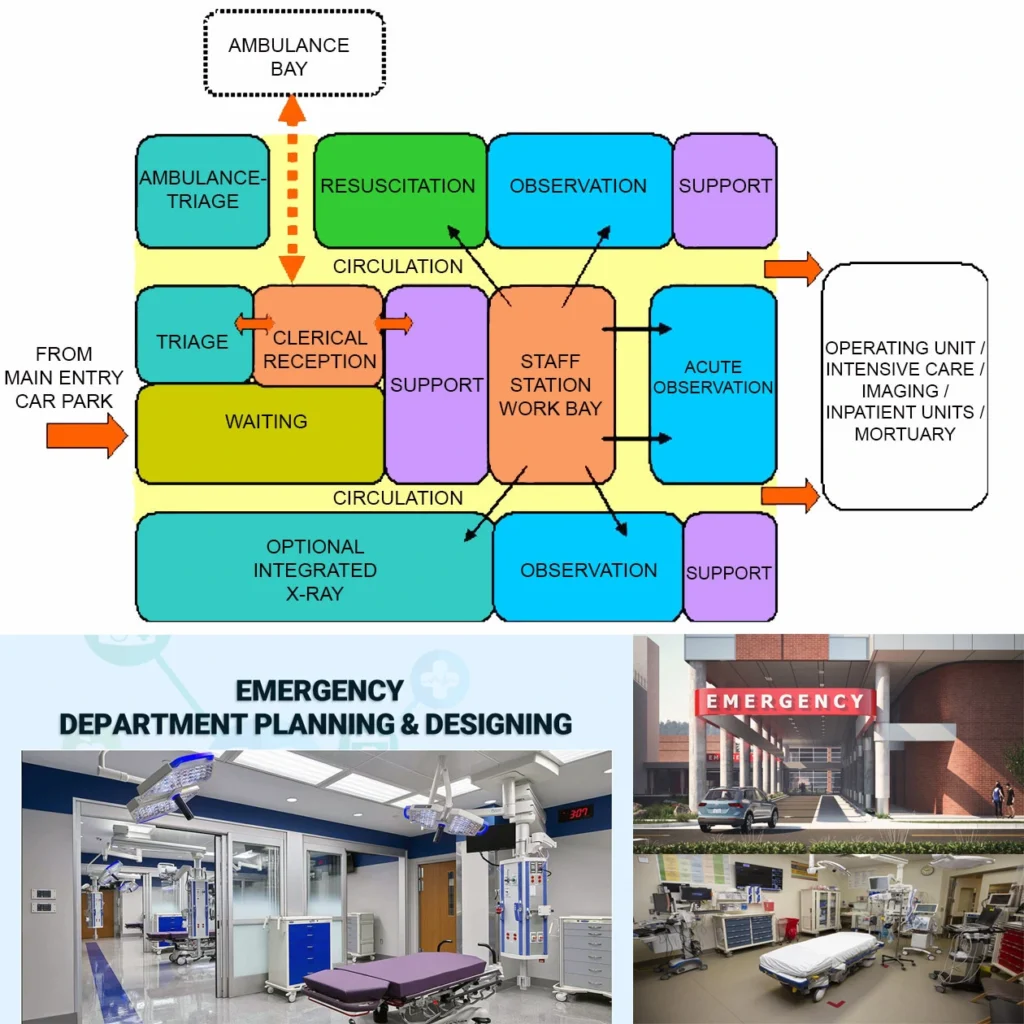
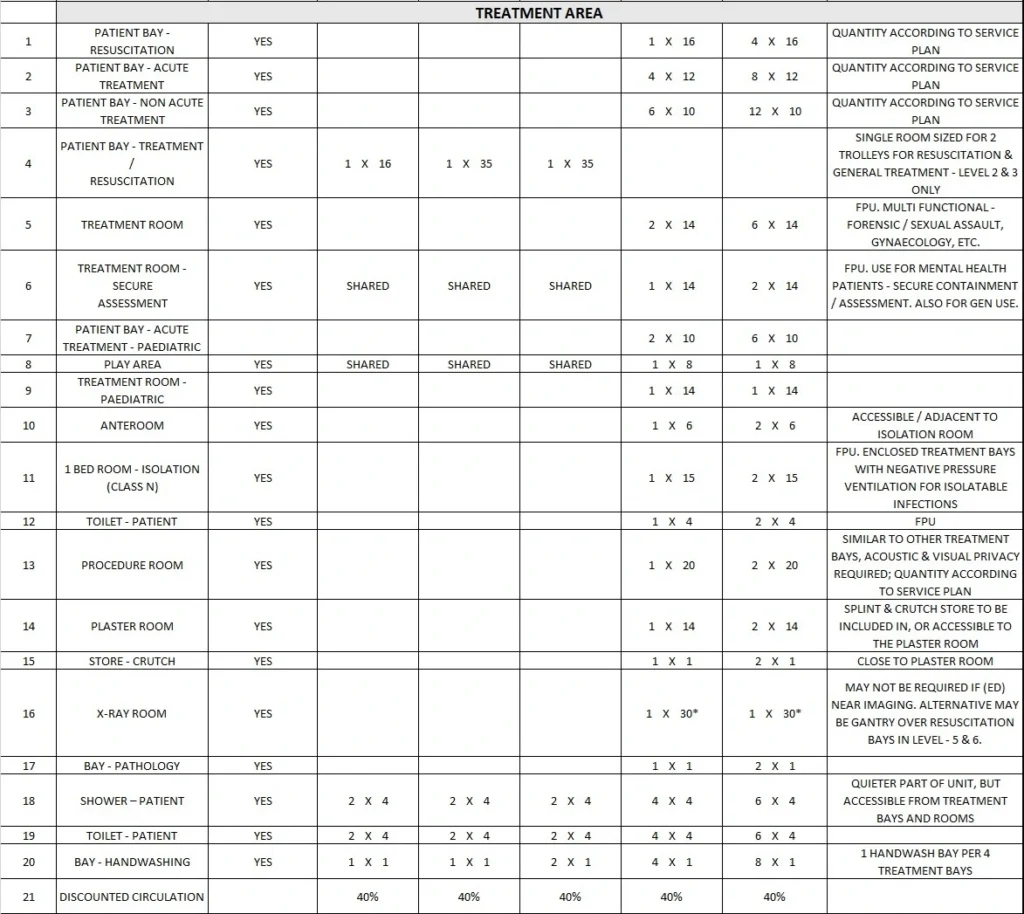
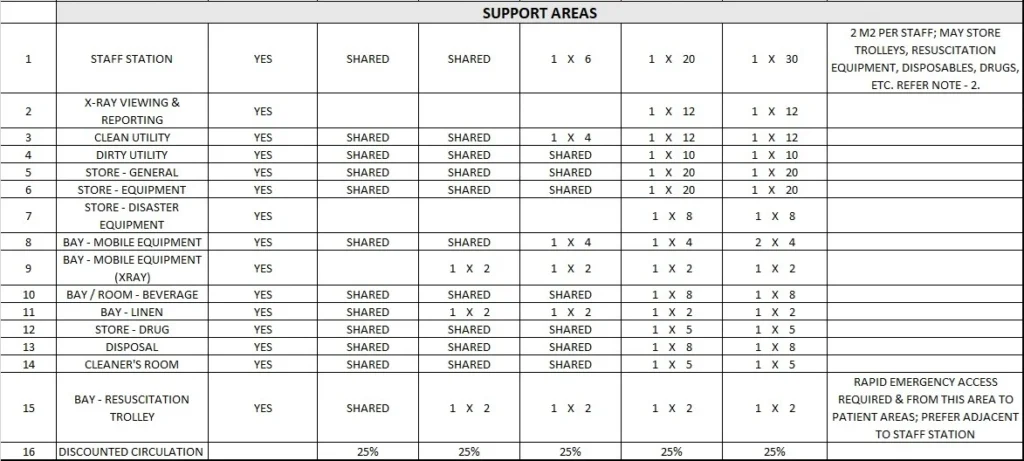
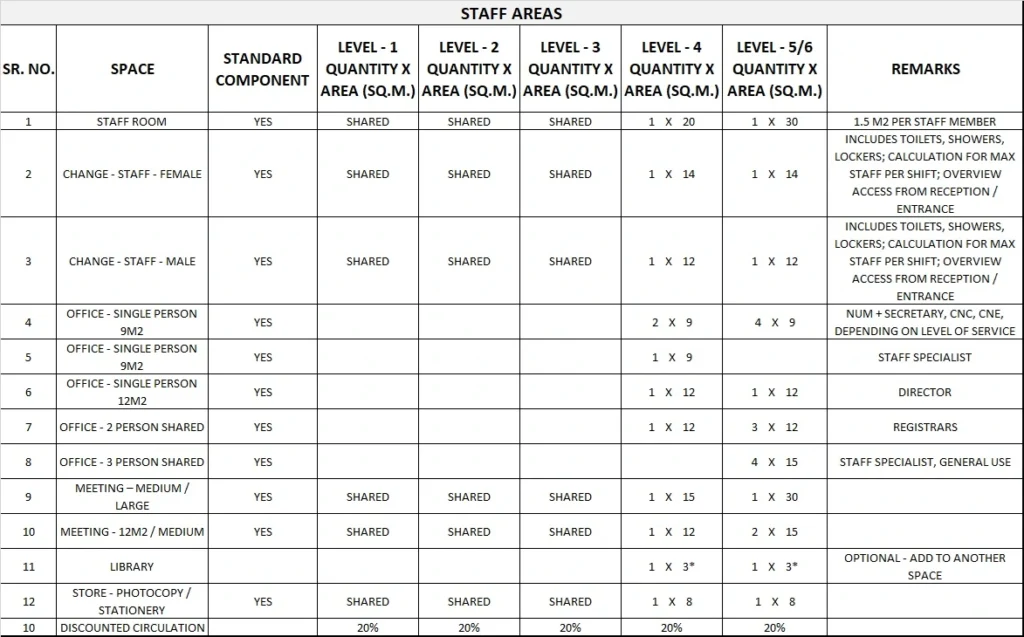
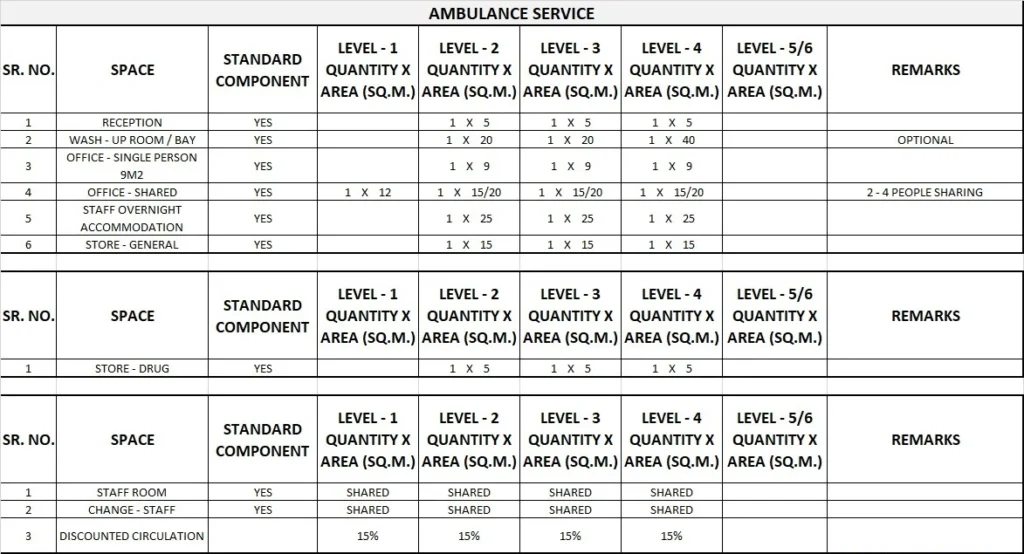
4) Schedule of Accommodation
Emergency Unit Generic Schedule of Accommodation
Schedule of Accommodation for an Emergency Unit Levels 1 to 6.
Note 1:
Staff Station should be located centrally within Treatment Area, preferably with direct oversight of Resuscitation Bays. Direct access required to treatment spaces.
It may be raised for uninterrupted vision of the patients. It may be partially enclosed to ensure that confidential information can by conveyed without breach of privacy and to provide security to staff and confidential information.
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
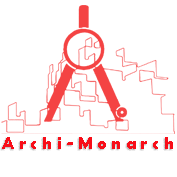
5) Functional Relationship Diagram
Emergency Unit Functional Relationship Diagram