An Adult Mental Health Inpatient Unit is a specialized medical facility designed to provide intensive care and treatment for individuals experiencing severe mental health crises.
These units offer a structured and supportive environment where patients receive round-the-clock care from mental health professionals, including psychiatrists, psychologists, nurses, and therapists.
The primary focus is to stabilize patients, address acute symptoms, and develop a comprehensive treatment plan for long-term recovery.
The Adult Acute Psychiatric Inpatient Unit provides assessment, admission and inpatient accommodation in a safe and therapeutic environment suitable for adult mental health patients and staff.
This section is applicable to:
- A stand alone Adult Acute Psychiatric Inpatient Unit or group of units
- A dedicated Adult Acute Psychiatric Inpatient Unit within a general hospital
- A number of dedicated Patient Bedrooms as an annexe to an Acute Inpatient Unit
The Operational Policy shall determine the size and function of the Adult Acute Psychiatric Inpatient Unit.
An Adult Acute Psychiatric Inpatient Unit shall comply with the requirements outlined for Inpatient Accommodation, but with the noted modifications or additions in this section.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Planning of AMHI Unit
i) Planning Models
Some patients may at times exhibit disturbed or high risk behaviour. Appropriate planning and use of materials (for example safety glass, low maintenance/ resilient surface etc) can achieve an environment where all patients can co-exist with minimal disruption to each other. The building should be able to accommodate patients of all levels of disturbance without taking on the characteristics of a jail.
Externally the principal concept of planning should be to integrate the new facility with its surrounds, and with the other buildings. Planning of external spaces must take into account the requirement for provision of a secure garden associated with the High Dependency area, and an open garden area for general use. The area should be based on 10 m2 per person.
The design of external spaces, as for the building, should be domestic in nature, rather than formal or monumental. They should have the following features:
- The building should consciously have a front and a back
- It should provide opportunities for privacy, recreation and self expression
- It should provide opportunities for movement/ambulation both indoors and outdoors with unobtrusive environmental boundaries and with appropriate safety provisions
- Single rooms are recommended.
Rooms may be grouped into clusters that can be defined for distinct patient groups; each cluster of rooms should include a recreational space to allow for patient therapy and flexibility for a variety of patient categories.
Additional considerations include:
- Flexibility of space usage through consideration of a range of patient needs for personal and shared space
- Clearly defined patient residential areas readily identifiable by patients who may be disoriented or disturbed
- An effective balance between opportunities for patients’ privacy and the need for staff to observe patient behaviours.
ii) Functional Areas
The Adult Acute Psychiatric Inpatient Unit will consist of a number of functional areas or zones as follows:
- Main Entry/ Reception / Clerical area
- Assessment/ Procedural area
- Staff Offices/ Administrative and management area
- Staff Amenities area
- Inpatient Area including outdoor areas
- Secure Area including secured courtyard
Administration and office areas
The Unit Manager’s Office should be located in, or directly adjacent to the patient area and in particular, the Staff Station. There should be the capacity to control patient’s access to administrative and office areas.
There may be a requirement for a communication system between interview areas and the Staff Station to signal the need for assistance. There should be provision for a Secure Store as part of the Group/View Room to house audio-visual equipment.
Admissions area
The Admissions area will comprise an Admission Office, general purpose Interview Room and Examination Room and will be used by nursing, allied health and medical staff to interview relatives/ patients. Examination and consultation of patients will be carried out in these areas.
Duress alarms are required in all these areas. The Admissions Area should be directly screened from the Waiting Area. Noise transmission between these rooms and the waiting area should be reduced to a minimum so that conversations are not overheard.
Day rooms
At least two separate social spaces shall be provided, one for quiet activities and one appropriate for noisy activities.
Drug dispensing / storage
The Drug Distribution Station shall include extra provision for security against unauthorised access.
ECT Facilities
ECT procedures should be undertaken in the Day Procedures Unit, ECT Suite or Operating Unit.
Ensuites
Each bedroom in the open unit is to have its own ensuite. There are a number of configurations – inboard, outboard and between rooms. The latter option is preferred as it maximises bedroom use and patient observation.
The inboard option provides privacy and dignity but should be used with caution for the following reasons:
- a narrow passage may be created at the entrance to the bedroom that may limit observation through the door vision panel
- blind spots may be created inside the bedroom, facilitate barricading
- staff attending any emergencies in the room must enter in single file
The door to ensuites should open in a way to avoid creating a blind spot when open or – with inboard ensuites – enable the ensuite door and bedroom door to be tied together to create a barricade. Ensuite doors are to be lockable by staff when needed and have a privacy latch that can be opened by staff in an emergency.
Entry areas
The Entrance provides direct access to the unit for patients referred for admission arriving either with relatives, via police or ambulance and alternative access to the unit for patients arriving via the Emergency Unit of the main hospital.
Provision should be made for a gun safe that allows Police to deposit firearms when they are in attendance at the Inpatient Unit.
The Emergency Entrance should be capable of direct approach by ambulance/ police vehicles and should have sufficient shelter to allow transfer of patients in shelter from the elements. The Entrance should have an airlock capable of accepting an ambulance trolley with ease.
There should be provision for an intercom between the Emergency Entrance and the Staff Station. The Entrance Area zone of the building should attempt to break down the ‘threshold’ feeling of many institutional buildings, while maintaining a sense of direction to the approach.
Group therapy area
Space for group therapy shall be provided. This may be combined with the quiet Day Room provided that an additional 0.7 m2 per patient is added and a minimum room area of 21 m2, enclosed for privacy, is available for therapy activities.
Secure area – high dependency / seclusion / intensive care
The High Dependency/ Intensive Care bedrooms must be lockable and able to be opened from the corridor should a patient attempt to blockade themselves in the room. Doors require a viewing panel, positioned to ensure that should the glass be broken or removed, a patient cannot put an arm through and operate the door lock. High Dependency bedrooms may be accessible to both the low dependency and high dependency sections of the unit. The High Dependency/ Intensive Care Areas will require access to a Seclusion Room.
These zones should be capable of secure separation from the remainder of the unit. There should be defined areas for male and female patients The High Dependency Unit, for client and staff safety purposes, should back onto the Staff Station to ensure easy visibility of the interior of the High Dependency Unit and rapid response in times of patient emergency. Patients in this area will require access to a secured courtyard.
Inpatient areas
Single bedrooms
An external outlook coupled with high ceilings adds to the perception of light and space and is a positive contribution to treatment. There should be no ‘blind spots’ in the rooms particularly any created by open doors and the rooms should be key-lockable from the outside.
Doors should be able to be opened from the corridor should a patient attempt to blockade him/herself in the room. Door viewing panels are optional in open unit bedrooms and will be dependent on the Unit’s Operational Policy. Low wattage night light over the bed space for use by staff when carrying out night time observations of patients should be considered.
Acoustic treatment to bedrooms is required to minimise transference of noise between adjoining bedrooms. Whilst domestic-style beds may be preferred for ambience, consideration should be given to occupational health and safety issues of staff attending to low height beds.
Two bed rooms
Two bed rooms may be included in the General Inpatient Zone providing an option for sharing, or provide accommodation of a mother and child. They can however be restrictive, result in the disruptive movement of patients to other rooms in order to accommodate new admissions and are generally not recommended.
Occupational therapy area
Each Adult Acute Psychiatric Inpatient Unit shall contain 1.5 m2 of separate space per patient for Occupational Therapy with a minimum total area of 20.0 m2.
The space shall include provisions for:
- Hand-washing
- Workbenches
- Storage
- Displays.
Occupational Therapy Areas may serve more than one Inpatient Unit.
iii) Functional Relationships
The Adult Acute Psychiatric Inpatient Unit should be located with ready access to the Emergency Unit, Main Entry and service and support areas including Catering Unit, Cleaning/ Housekeeping, Linen Handling, Waste Management and Supply Unit.
2) Design of AMHI Unit
i) Environmental Considerations
Acoustics
Acoustic treatment should be applied to the following areas:
- Day Areas such as patient living, dining and activities areas
- Patient Bedrooms including high dependency, intensive care and seclusion rooms
- Consulting Rooms
- Admission Areas.
In acoustically treated rooms, return air grilles should be acoustically treated to avoid transfer of conversations to adjacent areas. Door grilles to these areas should be avoided.
Windows and glazing
Wherever possible, the use of natural light is to be maximised. For glazing, graduate the impact resistance of the glass from toughest at lower level to weakest at high level. In areas where damage to glass may be expected, avoid larger pane sizes. Smaller panes are inherently stronger for a given thickness than larger panes.
Where toughened glass is used it should be treated with a protective film to ensure glass is held together when broken. Laminated / toughened glass of various thicknesses should be installed dependent upon the likelihood of patient injury or building damage.
All windows and observation panels shall be glazed with safety glass. Polycarbonate is not recommended due to surface scratching which will reduce visibility over time. Where windows are openable, effective security features such as narrow windows that will not allow patient escape, shall be provided. Locks, under the control of staff, shall be fitted.
ii) Space Standards and Components
Size of unit
The schedule of accommodation has been developed for typical 20 and 30 Bed Adult Acute Psychiatric Inpatient Units. For alternative configurations, allocate space for key areas according to the following guide:
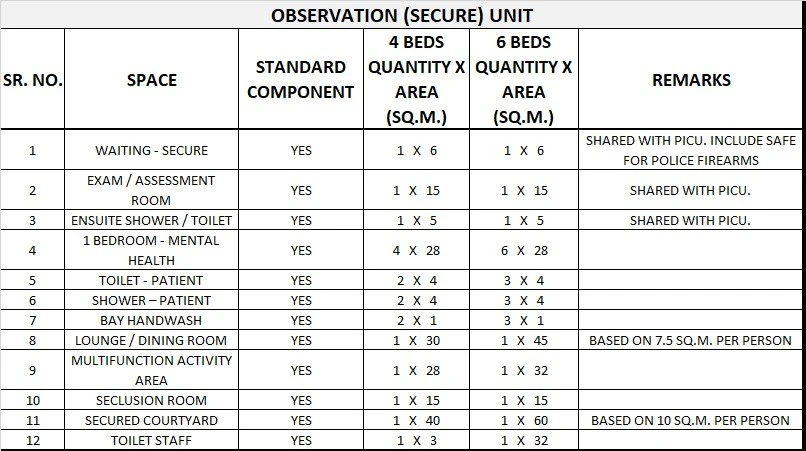
- Lounge/dining/activity areas – Secure Observation – 7.5m2 per person
- Lounge/dining/activity areas – General – 5.5m2 per person
- Outdoor areas (courtyards and terraces) – Secure – 10m2 per person
- Outdoor areas (courtyards and terraces) – General – 5m2 per person
- Courtyard and Terrace – minimum area – 20m2
- Consultation rooms – 1 per 5 beds
- Examination/assessment rooms – 1-2 per unit
iii) Safety and Security
Security within the facility and the surrounding outdoor area, related to patient movement requires careful consideration and may include use of video surveillance and motion sensors. The security of access for staff, community and domestic service deliveries should also be considered.
The design should assist staff to carry out their duties safely and to supervise patients by allowing or restricting access to areas in a manner which is consistent with patient needs/skills. Staff should be able to view patient movements and activities as naturally as possible, whenever necessary.
Controlled and/or concealed access will be required as an option in a number of functional areas. Functionally the only difference between an open and a closed (locked) area in their design should be the provision of controls over the flow to, from and throughout the facility.
Such controls should be as unobtrusive as possible. A communication system which enables staff to signal for assistance from other staff should be included.
iv) Finishes
The aesthetics are to be warm and user-friendly wherever possible.
v) Fixtures and Fittings
Fixtures and fittings should be safe and durable. Generally, all fixings should be heavy duty, concealed, and where exposed, tamper proof. Fittings, including hooks, curtain tracks, bathroom fittings, should be plastic where possible, and have a breaking strain of not more than 15kgs.
Fittings should avoid the potential to be used either as a weapon or to inflict personal damage. Paintings, mirrors and signage should be rigidly fixed to walls with tamper proof fixings. Mirrors shall be of safety glass or other appropriate impact resistant and shatterproof construction. They shall be fully glued to a backing to prevent availability of loose fragments of broken glass.
Holland blinds, Venetian blinds and curtains should be avoided in patient areas. Curtain tracks, pelmets and other fittings that provide potential for patients to hang themselves should be avoided or designed so that the potential is removed.
vi) Building Services
Avoid exposed services, for example, sink wastes which may be easily damaged.
Light fittings, smoke detectors, thermal detectors and air-conditioning vents to higher dependent areas, particularly Seclusion Rooms, should be vandal proof and incapable of supporting a patient’s weight.
3) Components of the Unit
The Adult Acute Psychiatric Inpatient Unit will consist of a combination of Standard Components and Non-Standard Components.
Provide the Standard Components as identified in the Schedule of Accommodation and to comply with details in Standard Components described in these Guidelines.
i) Non Standard Components
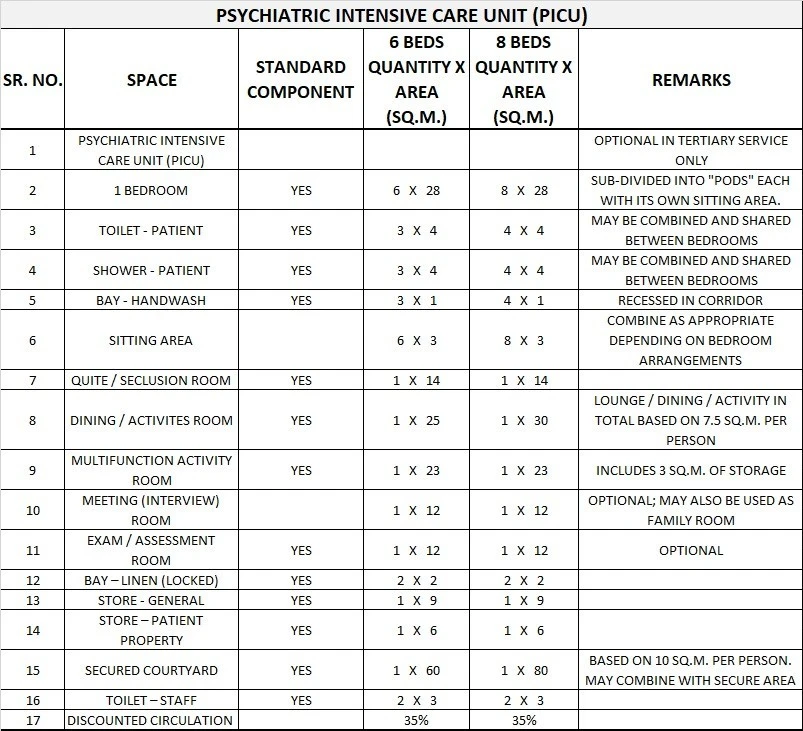
Sitting area (PICU)
Description and Function – A small sitting area may be provided for the use of patients, external to secure bedroom areas for PICU patients. Sitting areas need to be under direct observation of staff.
Location and Relationships – Locate in the PICU secured zone, adjacent to the bedroom, with direct observation of staff.
Considerations – Furniture is to be soft, foam type to prevent harm to patients and avoid being used as an implement.
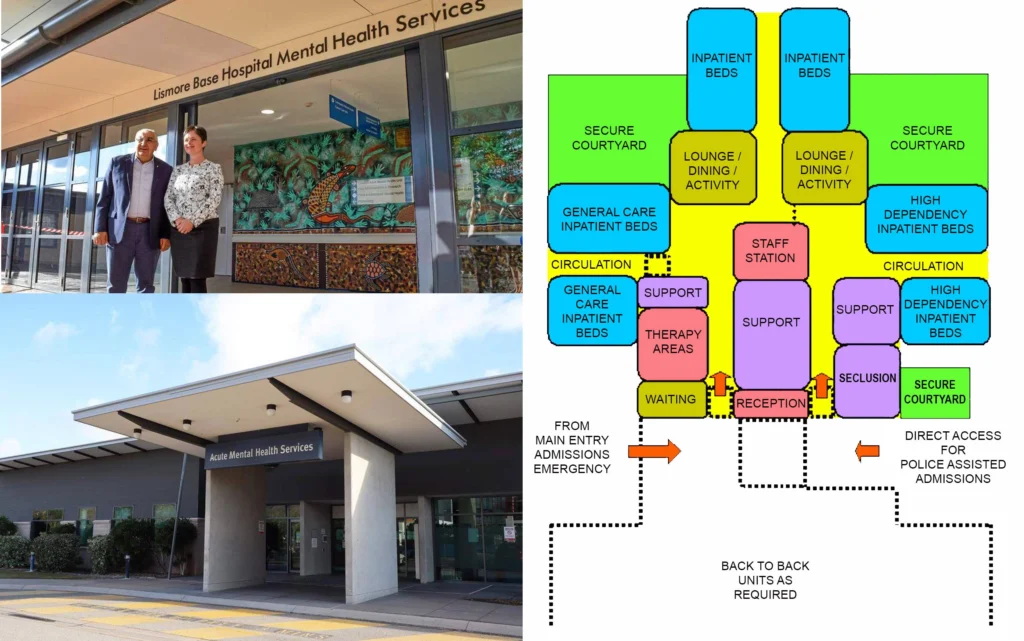
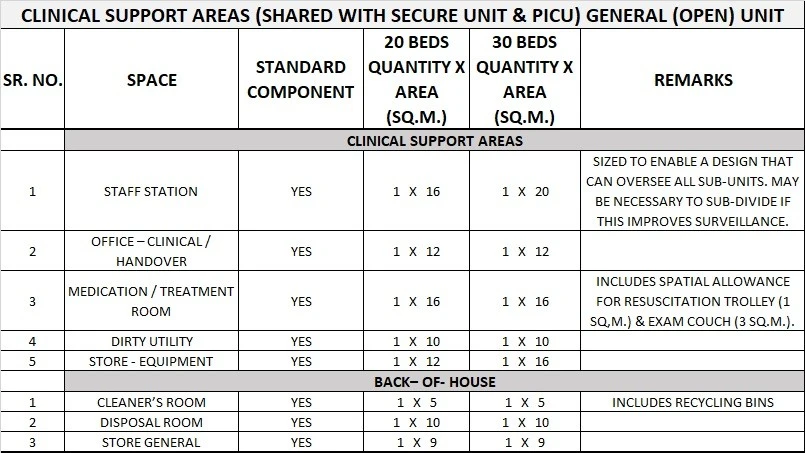
4) Schedule of Accommodation
Adult Mental Health Inpatient Unit Generic Schedule Of Accommodation
Schedule of Accommodation for an Adult Mental Health Inpatient Unit with 20 Beds and 30 Beds.
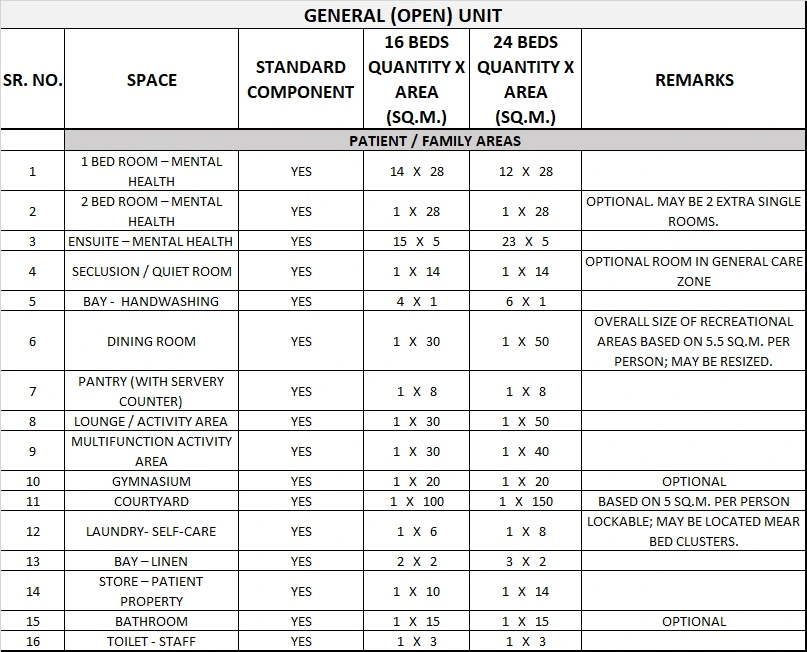
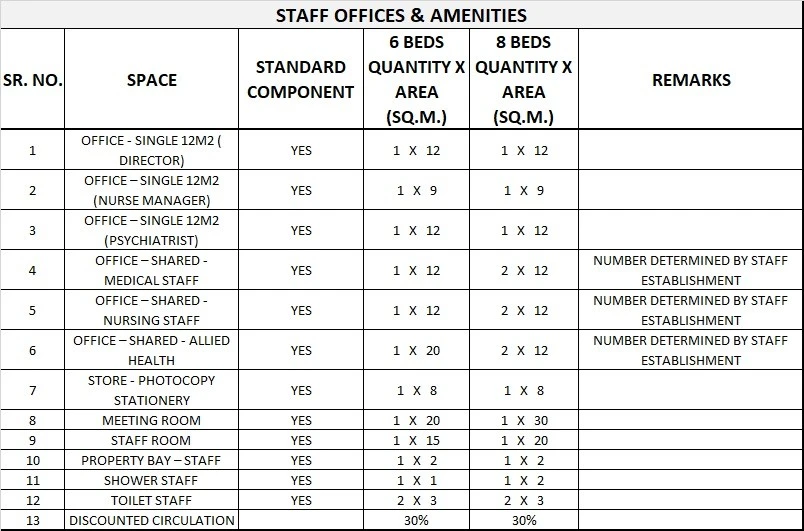
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
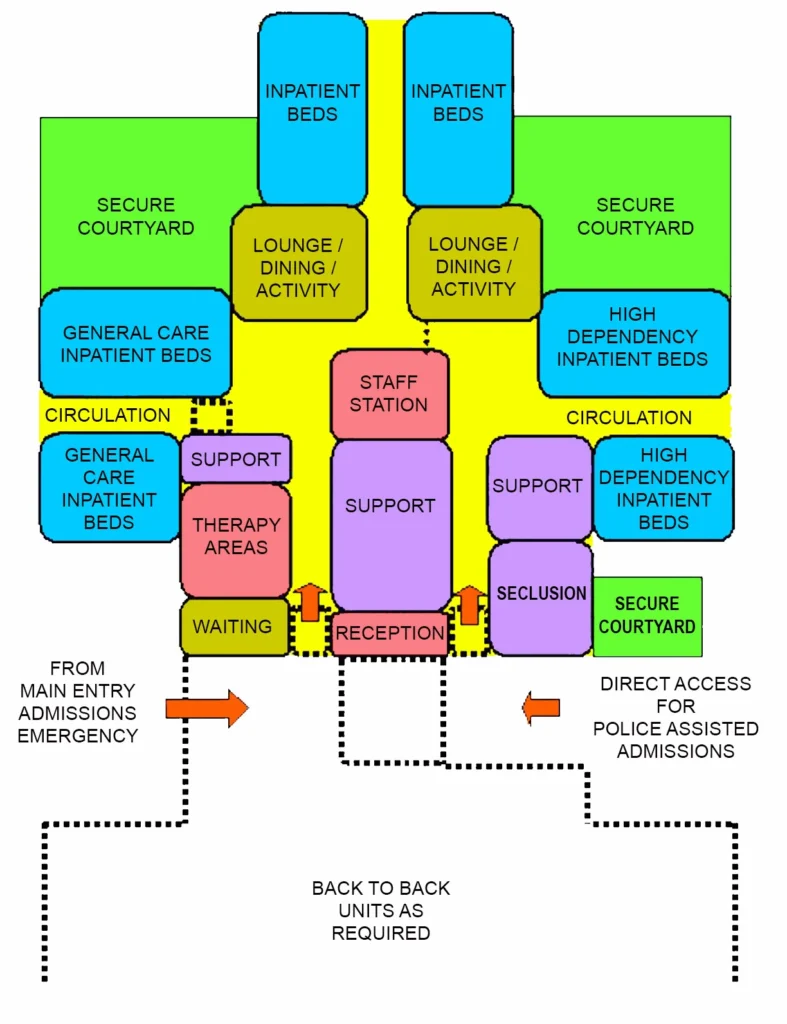
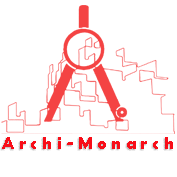
5) Functional Relationship Diagram
Adult Mental Health Inpatient Unit Functional Relationship Diagram