An obstetrics unit—often referred to as a maternity ward or labor and delivery unit—is a specialized section within a healthcare facility dedicated to the care of women during pregnancy, childbirth, and the immediate postpartum period.
These units typically include spaces for labor, delivery, recovery, and postpartum care (commonly known as LDRP or LDR units), and may also be connected to neonatal intensive care units (NICUs) for infants who require specialized care.
The unit’s main functions revolve around ensuring the safe delivery of babies, providing medical support to mothers and newborns, and offering a comfortable, supportive environment for families during one of life’s most significant moments.
Why Design Matters in Obstetrics Units
The design of an obstetrics unit plays a crucial role in shaping the quality of maternal care, the efficiency of healthcare delivery, and the experience of patients and staff alike.
Poorly designed spaces can contribute to workflow inefficiencies, increase the risk of infections, and cause emotional discomfort for mothers and families.
A well-designed obstetrics unit should:
- Ensure patient safety through smart layout and infection control.
- Support efficient clinical workflow for doctors, nurses, and midwives.
- Foster a calm, private, and emotionally supportive environment for laboring mothers.
- Facilitate flexibility to accommodate various birthing preferences and emergency situations.
In essence, thoughtful design improves not just clinical outcomes, but also emotional experiences—making it a cornerstone of patient-centered care.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
The Obstetric Unit is a discreet Unit providing facilities for the safe prenatal care, delivery and post natal care of mothers and their babies. The number of birthing preparation rooms and the size of the associated service areas shall be as required by the proposed obstetrical workload as outlined in the Operational Policy.
The exact scope of the unit is described in the Role Delineation Level which allows for 4 different levels at which the unit can operate. The description of the unit within this Guideline is based on a Level 4 unit which typically suits patients (both mothers and babies) with low to medium risk factors and associated complications.
It caters for approximately 1000 deliveries per annum and is based on 24 patient beds, 4 birthing rooms and a special care nursery. Within the unit, patients with specific needs will be taken into consideration through the creation of dedicated zones:
- Mothers having normal deliveries
- Mothers suffering from antenatal or postnatal complications, requiring acute maternity care
- Babies requiring minimal care
- Babies requiring care for complications arising from medium risk factors
- Babies requiring care for severe complications, in anticipation of a transfer to a Neonatal Unit of a higher delineation.
It is expected the Obstetric Unit, including the nursery, will be managed as one unit.
2) Planning of Obstetric Unit
i) Planning Models
Obstetrics consists of the following processes:
- Labour
- Delivery/ Birthing
- Recovery
- Postnatal (or Post-Partum)
- Separate from these 4 processes, the baby infant nurseries
A traditional Obstetrical model is based on the patient being moved between areas dedicated to the individual processes. The preferred design for an Obstetric Unit however, particularly for smaller birthing centres, includes a number of self contained rooms fitted out to perform several of the processes, without the patient having to move according to the following:
- The design model combining labour, delivery and recovery in one room will be referred to as an LDR model. The patient is only moved from this room in case of complications (to the Caesarean section delivery room) or after recover, to an in-patient room.
- The design model combining all four processes will be referred to as LDRP model. Here the patient remains in one room for her entire stay.
Larger birthing centres may adopt a more traditional model where dedicated maternity inpatient beds are provided, combined with a separate birthing suite. If the birthing centre does not provide a stand alone Special Care Nursery or Neonatal Intensive Care Unit, a Level 1 nursery may be provided.
ii) Functional Areas
The Obstetric Unit consists of the following functional areas:
- Reception and arrival area including provisions for visitors and administrative activities
- Inpatient areas for general mother care and for acute care (both antenatal and post natal)
- Birthing areas
- Neonatal Nursery area – General Care Nursery area
- Shared support and staff areas including facilities that can be shared between zones or Units.
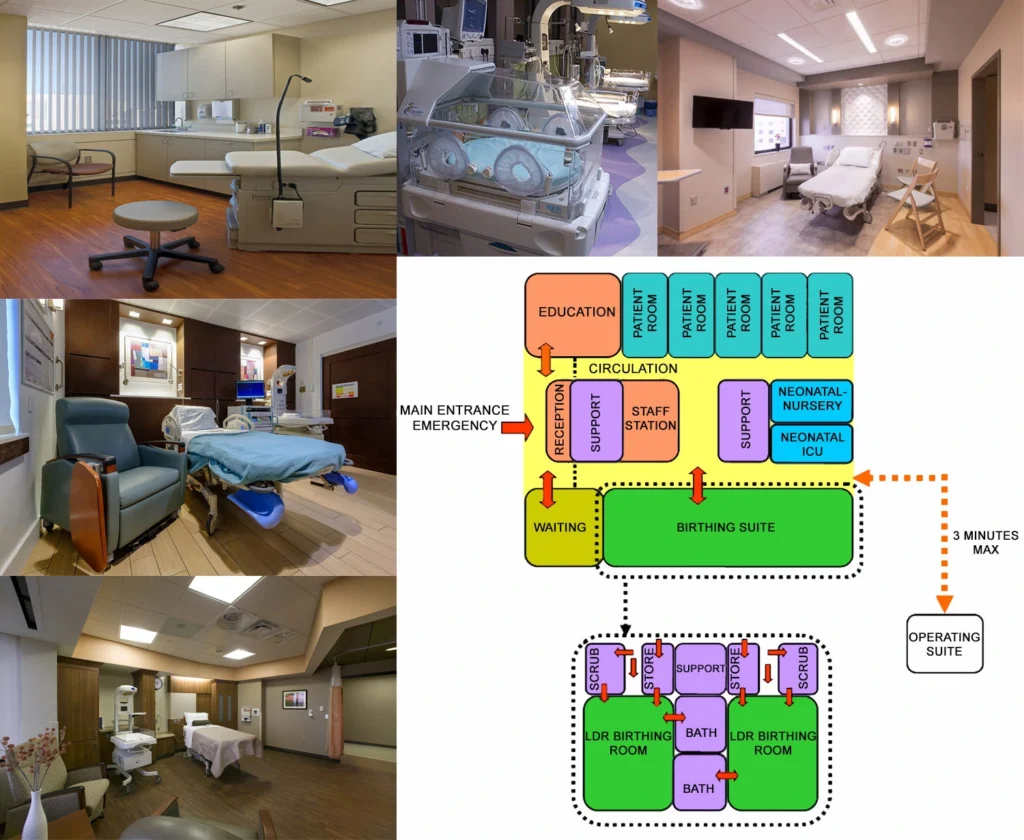
The Obstetric Unit will require rapid access to Operating Unit for emergency Caesarean Section deliveries; the Operational Policy will determine the requirement for Operating facilities located within the Birthing Area.
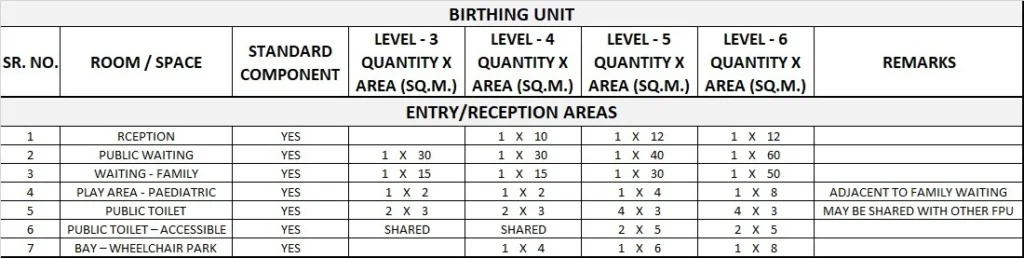
Reception Area
The reception is the receiving hub of the unit and should therefore ensure the security of the entire department through access control, duress alarm buttons as a minimum and baby tagging as a preferred option.
Mothers, their supporters and members of the public will need to have good access to public phones and separate male/female toilet facilities, prayer rooms (a minimum of 1 prayer room per sex, per floor) and waiting areas.
A separate waiting area for families should be provided too, preferably with a small play area for children. Considering the substantial volume of flowers and gifts delivered to the unit, secure holding space should be provided adjacent the reception.
The reception may be used for the registration of expectant mothers; alternatively this can occur within the maternity ambulatory care area. Good access from reception to the nursing administration offices and education areas is beneficial.
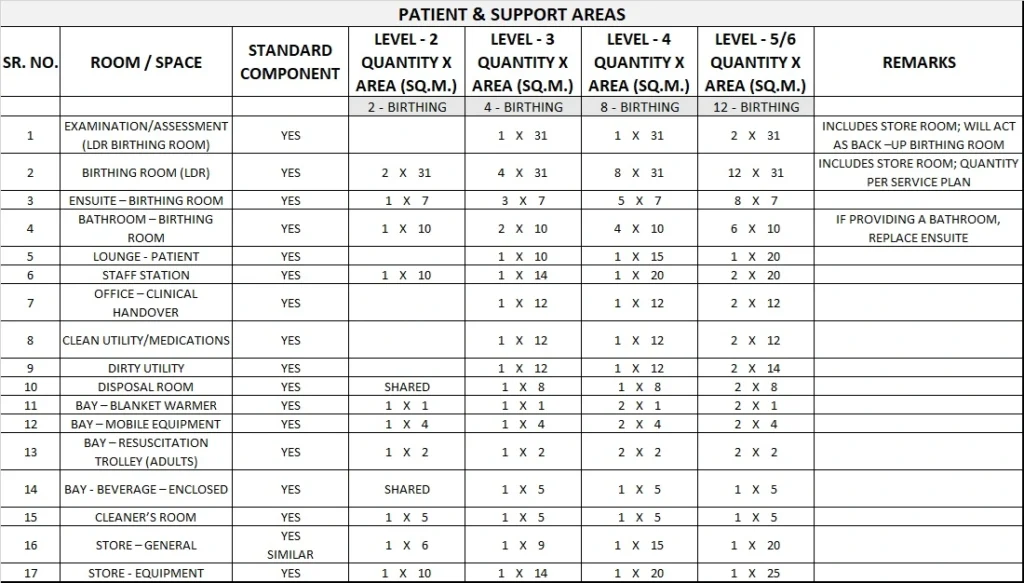
Inpatient Area
The inpatient area shall cater for both antenatal and postnatal patients. Although the unit described under this section is based on 24 patient beds – preferably only single rooms, for acute care and mother care – the bed numbers and mix will ultimately be determined by specific service conditions such as patient demographics, operational policies, cultural issues
etc.
Mother care areas shall be designed to suit mothers and babies who are well whereas the acute care area shall cater for antenatal patients, post natal patients with complications or simply for mothers recovering from Caesarean sections.
Patient rooms shall be grouped together in zones corresponding to their different levels of dependency. The more relaxed environment of mother care rooms can be located further away from the staff observation posts and the support areas whereas the more clinical acute care rooms shall be located to allow for effective staff observation and ease of access from the support areas. With regards to the different type of rooms:
- Due to requirement for a high level of privacy, the use of double rooms should be avoided unless specifically requested by the operator.
- Subject to the level of service provided and the likelihood of contagious diseases in the population, a pair of adjoining negative pressure isolation rooms with anterooms shall be provided.
Birthing Area
The birthing area caters for all the processes surrounding the birth of a newborn: assessment, labour, delivery (with/without intervention), bonding between mother (and the greater family) and child, resting and recovery and finally, the transfer to an inpatient unit or a discharge in case of a community midwifery programme. Where the LDRP model is followed, obviously
most of these processes will be taking place in one dedicated room.
An Obstetric Unit shall have:
- Birthing rooms, typically , LDR type
- At least 1 multi-purpose assessment room for consultations, examinations and if required, for delivery.
- Family/supporters facilities, allowing them to take part of the entire birthing process
If water birthing is included in the Operational Policy, the Unit will require access to a dedicated Bathroom. The Bathroom will require a large peninsular bath, with access to both sides of the bath. The Bathroom shall have a minimum area of 10 m2 and comply with all other requirements noted in Standard Components – Bathroom.
Note: These Guidelines do not imply endorsement of Water Birthing as a safe or appropriate operational model.
Nursery Area
A Level 1 nursery (General Care) could be provided as a supplementary area to the maternity inpatient area, under a level 3 or 4 Obstetrics Unit. The general care nursery will provide for the general care of healthy babies, such as:
- Feeding the baby
- Bathing, changing and weighing the baby
- Allowing the baby to sleep during the day in blacked out conditions
- Provide education to staff and parents
- Phototherapy
- Short term care, including the provision of assisted ventilation, for babies who suffer from complications and while they are waiting to be transferred to a neonatal intensive care unit/facility.
The general nursery should allow for cot spaces to comply with Standard Components; the clear space between the cots should be at least 1 metre. The number of cots will depend on the rooming-in policy of the facility and/or the statistics on how many mothers prefer/are able to proceed with rooming-in.
A Level 2 nursery (Special Care) will provide similar care as a Level 1 but also cater for premature newborns who are ill or who are simply recovering. Due to their prematurity and/or low weight, they will be cared for in humidicribs and bassinettes.
Shared Support and Staff Area
Like elsewhere in the facility, sharing space, equipment and staffing should be promoted, both within the unit and with other units. Within the unit sharing of staff stations, support and waiting areas should be possible between the different zones.
Toilet facilities, prayer rooms and educational spaces could be shared with other units. Obviously, where spaces are shared, the size should be increased proportionally.
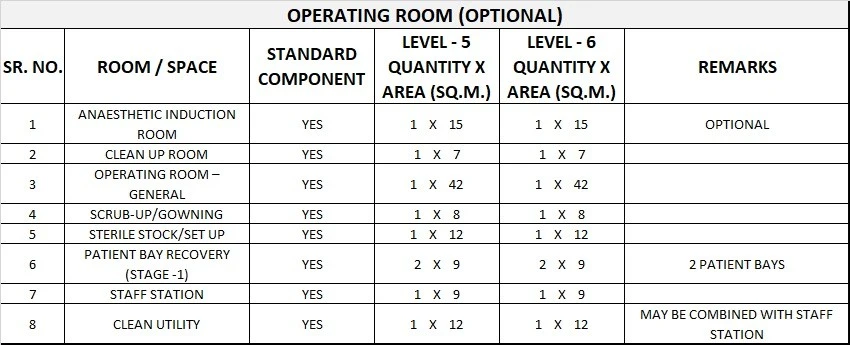
Operating Room/s and Support Facilities
If provided within the Obstetric Unit, Operating Room and support rooms shall have:
- Operating Room to comply with Standard Components – Operating Room, General; provision should be made for twin baby resuscitation areas within the operating room
- Scrub-up/ Gowning Bay to comply with Standard Components Scrub-up/ Gowning, 6 m2
- Clean-up Room
- Two Patient Bed Bays for Recovery for each Operating Room, to comply with Standard Components Patient Bay, Recovery Stage 1.
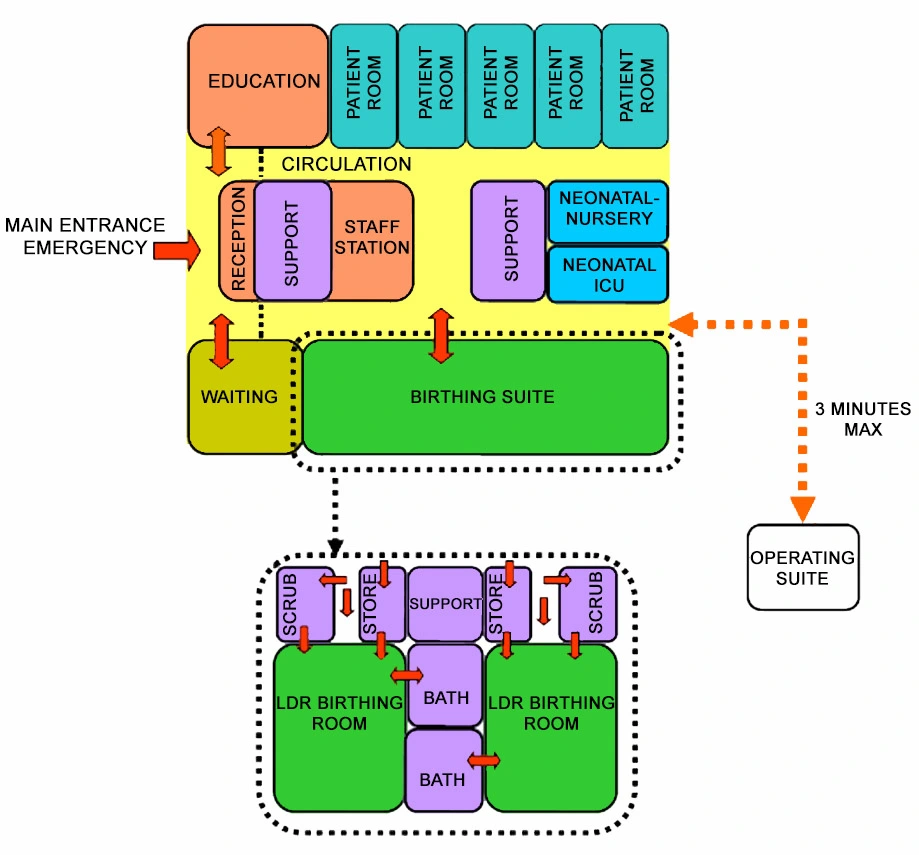
The time taken to travel to the Operating Room from the Birthing area ideally should not exceed three minutes. An assessment of the distance between the Birthing area and the Operating Rooms should be done taking into consideration the average speed of travel and whether lifts are involved including any delays associated with lift travel.
iii) Functional Relationships
External
The Obstetric Unit shall be located and designed to prohibit non-related traffic through the unit. When Birthing and Operating Rooms are in close proximity, access and service arrangements shall be such that neither staff nor patients need to travel through one area to reach the other.
It is highly desirable that, if an Intensive Care facility is to be provided for Obstetric use, it should be located as near as possible to the Obstetric Unit.
The unit should be in close proximity to:
- short term parking/drop off bay for dropping off expectant mothers
- hospital car parking and public transport access points
- flower delivery car parking bay
- ambulance transport parking bay
- helipad
Internal
The entrance to the unit shall provide direct access to the reception area. Adjacent to reception, areas are required for waiting including families. From there, direct access to assessment/ consultation/ examination, nursery, inpatient and birthing areas shall be provided.
Direct access to a climate controlled internal garden or courtyard for mothers and their supporters would be beneficial. Refer to the attached Functional Relationship Diagram.
3) Design of Obstetric Unit
i) General
The Obstetric Unit shall be located and designed to prohibit non-related traffic through the unit. When Birthing and Operating Rooms are in close proximity, access and service arrangements shall be such that neither staff nor patients need to travel through one area to reach the other.
It is highly desirable that, if an Intensive Care facility is to be provided for Obstetric use, then it be located as near as possible to the Obstetric Unit.
ii) Environmental Considerations
Natural Light
Essential to all patient rooms (mothers and babies).
Privacy
Privacy is essential for both the assessment and birthing rooms. Avoid direct views into the room from the outside, both through the windows and through the door – i.e. do not provide viewing panels and a privacy curtain should be allowed for. Furthermore, the foot end of the bed should be facing away from the door or the access point.
Acoustics
Within the nursery, sound absorption and insulation techniques should be applied to soften the noise created by crying babies and their support equipment. This however should not impede the quality of observation or ease of access between staff/support areas and the nursery.
Similar techniques should be applied to the birthing rooms, allowing mothers to give birth without disturbing other patients. The unit in general should be isolated from disturbing sounds of traffic and sirens of ambulances, either through its strategic location or through applying sound absorption and insulation techniques. Refer to Part C of these Guidelines for more information.
iii) Space Standards and Components
Doors
Appropriately sized and located doors shall be provided for emergency bed transfer to the Birthing or Operating Units. Also refer to Part C of these Guidelines.
Ergonomics
Refer to Part C of these Guidelines for more information.
iv) Safety and Security
The number of access points to the unit should be minimised. All entries should be under direct control of staff and while the daytime access is to be via the reception area, after hours access should give direct access to the birthing area.
As a minimum, this entry point should be fitted out with video intercom and remote access hardware, allowing for 24 hours access for expectant mothers, support persons of patients in the In-patient area or parents of neonates.
All entry points should also be controlled through an Access Control System – a combination of reed switches, electric strike/magnetic locks and card readers. Card readers should be provided on both sides of these entry points and these only should be deactivated in case of an emergency.
To increase the safety of newborns even further, the use of electronic tagging should be promoted. This involves a combination of the infant wearing a tag around the ankle and sensor panels located at every access point to the unit (and perhaps the entire hospital).
All reception areas and staff stations to have duress alarm buttons in obscure but easily accessible locations.
Where lifting devices are used for the baths within the birthing rooms, special attention should be given to the storage and handling of this equipment.
To ensure the correct milk is provided to the right infant, breast milk storage freezers and fridges should be lockable or located within a lockable formula room with access restricted to staff only or to mothers under staff supervision.
v) Finishes
A homely, non-clinical ambience is preferred for the nursery and birthing rooms. Medical equipment and services should be easily accessible but concealed behind built in joinery or screens.
Colours should be chosen carefully to avoid an adverse impact on the skin colour of patients and neonates, particularly of jaundiced babies. Refer to Part C of these Guidelines for more information on wall protection, floor finishes and ceiling finishes.
vi) Fixtures and Fittings
Refer to Part C of these Guidelines, the Room Layout Sheets (RLS) and Room Data Sheets (RDS) for more information.
vii) Building Service Requirements
Lighting
All High Dependency Care areas such as birthing suites (including bathroom/ ensuite), birthing/assessment rooms, nurseries and areas for the examination/resuscitation and bathing of babies are to have dimmable colour-corrected lighting.
HVAC
The birthing rooms and nurseries should be serviced by individual HVAC systems, allowing raising the temperature quickly to 25-27 degrees Celsius when a baby is born. The temperature control devices should be located within the room and should only be accessible to the staff.
Communications
All new phone, data and staff/emergency call systems should be compatible with hospital wide systems already in use. Annunciator panels should be located in strategic points within the hospital circulation area and should be of the “non-scrolling” type, allowing all calls to be displayed at the same time. The audible signal of these call systems should be controllable to ensure minimal disturbance to patients at night.
viii) Infection Control
Each birthing room should have a scrub basin. Each patient room should have a hand basin. Each pair of isolation rooms should have a hand basin outside.
Each nursery should have a hand basin at the point of entry, both for staff and parents. Within the nursery, minimum 1 hand basin should be provided per 6 cots and the distance between any point in the nursery to the closest basin should not exceed 6 metres.
The placenta is to be treated as contaminated waste and should be disposed of according to the correct waste management policy. Disposal using placental macerators is not appropriate and should be avoided. Freezer storage should be provided within the unit to allow for collection by the family, for cultural reasons.
4) Components of the Unit
i) General
The Obstetric Unit will contain a combination of Standard Components and Non-Standard Components. Provide Standard Components to comply with details in the Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets.
ii) Non Standard Components
Bathing / Examination Room
Description and Function – This room is primarily used to teach parents baby bathing techniques and to examine the infant. Provide purpose-built baby baths for occupational health and safety reasons. Portable baths or bassinets may be used for demonstration purposes, generally within the patient room.
Location and Relationships – The Bathing/ Examination room may be provided as part of a nursery or a maternity inpatient unit.
Considerations – The room will require:
- Bench with inbuilt baby bath; consideration should be given to the bench height and the mounting of baby baths to ensure ease of access for staff and mothers
- Warm water supply to baby baths and sinks; controlled temperature range
- Overhead heating to baby bathing area (in addition to airconditioning to prevent babies becoming cold)
- Storage space for baby linen
- Baby scales and measuring equipment
- Lighting level in the baby bathing examination should permit the examination of baby skin tones
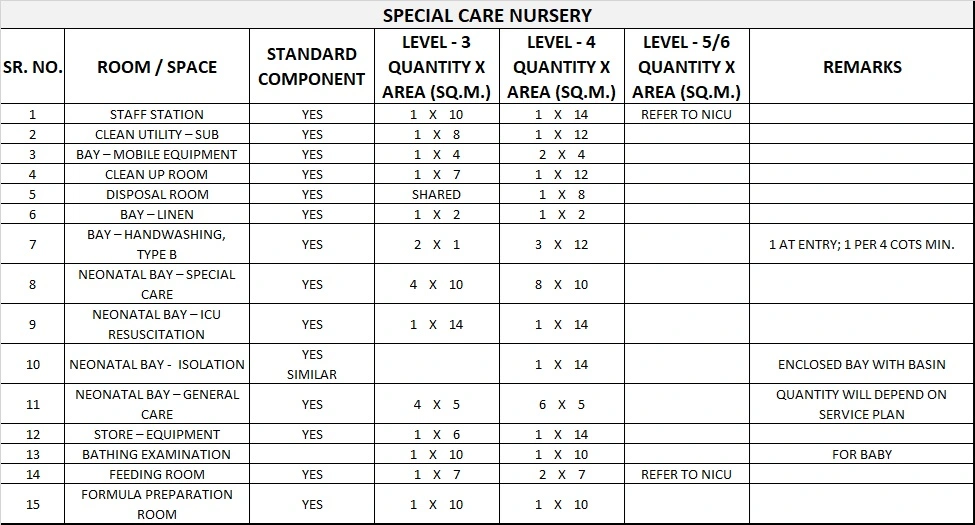
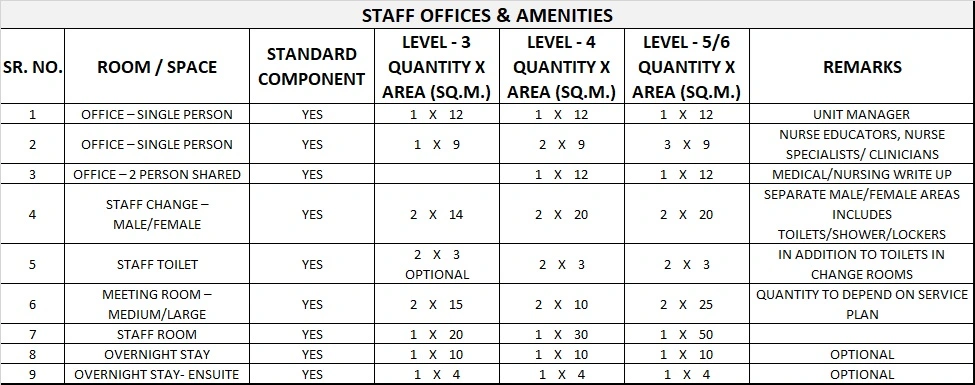
5) Schedule of Accommodation
Obstetrics Unit Generic Schedule of Accommodation
Schedule of Accommodation for an Obstetrics Unit for Level 3-6
Operating Room (Optional)
For emergency C-Sections only. Each Operating Room will require the following:
Notes:
Level 3 consists of 4 cot bays (typical). Quantity of cot bays will be determined by service plan
Level 4 consists of 8 cot bays (typical). Quantity of cot bays will be determined by service plan
Level 5 & 6; refer to NICU (Neo-natal ICU)
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
6) Functional Relationship Diagram
Obstetrics Unit Functional Relationship Diagram