Healthcare facility space design is a complex process that goes beyond aesthetics — it’s about creating an environment that supports healing, enhances operational efficiency, and ensures patient and staff safety. From hospitals to outpatient clinics, each facility has unique requirements that must balance functionality, patient comfort, and regulatory compliance.

Modern healthcare spaces need to be adaptable, ensuring they can accommodate technological advancements, changing patient needs, and evolving medical practices. Thoughtful design can transform a healthcare facility into a space that not only delivers medical care but also promotes a sense of calm and trust for patients and families.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Corridors
There are many schools of thought on minimum corridor widths and the underlying principles that should dictate them. The requirements set out in this section should be regarded as the minimum required.
These requirements take into account the need to allow for the movement of trolleys, beds, wheelchairs and other mobile equipment, including the passing of such equipment.
The overriding principle in setting the minimum corridor width is the need to allow for a workable width that, in the event of an emergency evacuation procedure, does not impede egress.
Note 1: Designers should note that other Building Codes might also specify minimum corridor widths for Patient Care Areas with a focus on Fire Safety or Disability Access. The requirements of these Guidelines for certain areas may be higher than codes such as Fire Safety since the subjects of concern are wider than those codes.
Note 2: Most large Hospital Units include a range of patient and staff-only corridors. If staff only areas are clearly designated by planning and are not required for patient access, then the guidelines for patient corridors do not apply.
Note 3: All corridor widths are clear of handrails and/or crash rails. It is recommended that for design purposes (and considering construction tolerances) 100 mm be allocated to each handrail.
In areas where patient beds, trolleys and stretchers will be moved regularly, such as Inpatient Units, Operating Units, Obstetric Units and Intensive Care Units, the minimum clear corridor width shall be 2300 mm.
The recommended corridor width in areas where there is frequent bed and trolley movement is 2400 mm. Even at this dimension, special consideration must be given to the width of doorways into adjacent rooms and widening corridors at the entry to the affected rooms to accommodate turning trolleys and beds.
Corridor widths in the above areas may be considered at lesser dimensions where an existing building is utilised, but special design and planning detail must be incorporated to overcome the problems of congestion and the potential risk to patients and staff in an emergency evacuation.
Note: In any event, any corridors that may be used by a patient for any purpose may not be narrower less than 1800 wide.
In areas where irregular trolley or bed movement is expected, such as Radiology, corridor widths can be reduced to 2000 mm. Special consideration must be given to the door widths to ensure the movement of trolleys or beds from corridor to adjacent rooms is not restricted.
In areas where there is no patient movement requirement and where corridor runs are no longer than 12 metres, such as a corridor to a group of staff offices, corridor widths of 1200 mm are acceptable.
Corridor widths of less than 1200 mm are unacceptable in patient care areas, except where forming part of an existing facility, and where written approval has been obtained for the lesser width.
The width of major inter-department arterial corridors and public corridors generally shall be as wide as is deemed necessary for the proposed traffic flow, but shall not be less that 2400 mm.
Note: In these Guidelines, the inter-departmental corridors are also referred to as ‘travel’.
Corridor widths shall mean clear, unobstructed widths. Items such as handrails, drinking fountains, hand basins, telephone booths, columns, vending machines and portable / mobile equipment of any type shall not reduce the minimum width or impede traffic flow.
Consideration shall be given to the elimination of potentially dangerous ‘blind spots’.
2) Ceiling Heights
The minimum acceptable ceiling height in occupied areas shall be 2400 mm, but consideration should be given to the size (aesthetic consideration) and use of the room.
A ceiling height of 2700 mm is considered more appropriate in work areas such as Therapy Rooms, Conference Rooms and Kitchens. Ceiling heights in Ensuite can be reduced to 2250 mm where required, to accommodate building services and structure.
Patient bed areas including bedrooms, ICU, CCU, HDU, Emergency, Recovery rooms and the like must be a minimum of 2700mm.
The minimum ceiling height in areas such as corridors, passages and recesses shall be 2400 mm. In portions of remodelled existing facilities, the corridor ceiling height may be reduced to 2250 mm, but only over limited areas such as where a mechanical duct passes over a corridor.
A reduced ceiling height for no greater corridor length than 3000 mm is acceptable. The extent of any such variation from the above recommendations must be approved in writing.
In areas where access is restricted such as a drinking fountain recess, a minimum ceiling height of 2250 mm is acceptable.
Rooms with ceiling mounted equipment, such as X-ray Rooms and Operating Rooms will require increased ceiling heights. Heights should comply with equipment manufacturers’ recommendations. Operating Room, Interventional Imaging rooms and Birthing room ceilings must be no less than 3000 mm.
Minimum ceiling (soffit) heights of external areas such as entry canopies, ambulance entries and delivery canopies should suit the requirements of the vehicles expected to use them.
Special consideration is to be given to the impact of whip aerials fitted to emergency vehicles. Ceiling heights in Plant Rooms are to suit the equipment and allow safe access for service and maintenance. The minimum recommended height is 2400 mm.
3) Department Sizes
Department sizes will depend upon the perceived facility role as set out in the Operational Policy and the organisation of services within the hospital.
Some functions may be combined or shared provided that the layout does not compromise safety standards and medical and nursing practices.
Note: Departmental sizes also depend on design efficiency. For guidelines on this subject refer to Efficiency Guidelines and Schedule of Circulation Percentages in this section.
4) Efficiency Guidelines
i) General
The concept of efficiency refers to the ratio between net Functional Areas and circulation space. Simplistic guidelines on efficiency tend to be misleading and should not be applied to vastly different functional briefs.
It is more appropriate to allocate different circulation percentages for generically different planning units. Such a guide has been provided under the Schedule of Circulation Percentages in this section.
Inadequate circulation allowance in briefing documents is not recommended. It can result in undue pressure on designers to reduce sizes and therefore functionality. It must also be noted that the circulation percentages are a guide only.
They apply to the Functional Planning Units (FPUs) included in these Guidelines under Generic Schedule of Finishes. For larger planning units, a different percentage may be appropriate.
ii) Net Functional Areas
In briefing documents, Net Functional Areas represent the sum of individual room areas without any corridors.
Refer to Part B – Planning: Area Measurement Methodology for a description of how to measure areas off the plans.
iii) Gross Departmental Areas
Gross Departmental Areas are calculated by adding the Net Functional Areas and departmental corridors. These are corridors that are entirely within one department (or FPU).
In calculating the departmental corridors the following should be taken into account:
- Service cupboards and passing risers are excluded.
- Corridor wall thicknesses are excluded as these are included in room areas.
- Columns are included.
- Fire stairs are excluded.
- Lifts and lift shafts are excluded.
iv) Travel
‘Travel’ represents arterial corridors that connect the FPUs. Travel is required to allow passage from one unit to another without going through the internal corridors of another FPU.
A target of 15 per cent is appropriate for Travel in a hospital of one to two storeys. Travel can be considerably reduced in high-rise buildings since in many instances corridors are replaced by vertical transportation.
In calculating travel, the following should be considered:
- Wall thicknesses are excluded as these are part of the Gross Departmental Areas
- Fire stairs are included once for each floor to floor connection
- External wall thicknesses are excluded
- Lift shafts are excluded
- Service cupboards are excluded
- Service shafts and risers are excluded
v) Engineering
Engineering refers to the area of Plant Rooms and other service areas. In calculating the Engineering allowance the following areas should be included:
- Service cupboards
- Lift motor rooms
- Service shafts and risers
Lift shafts should be excluded. The target of 15 % applied to Gross Departmental Areas may be used for a typical one to two storey hospital building.
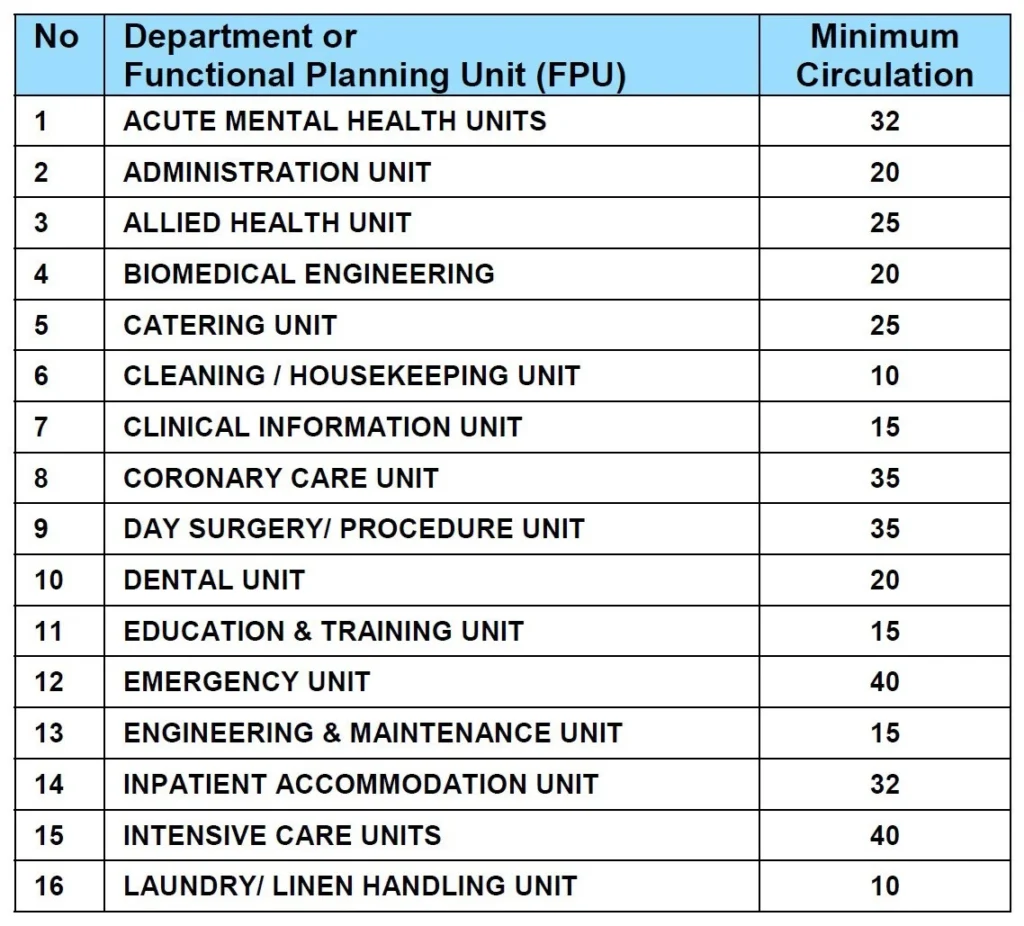
5) Schedule of Circulation Percentages
Recommended Circulation Percentages for typical Functional Planning Units (FPUs) are as follows: