An efficient medical records unit is a critical component of any healthcare facility, ensuring that patient information is accurately recorded, securely stored, and easily accessible to authorized personnel. Proper design and management of this unit directly impact patient care, legal compliance, and overall hospital efficiency.
The Role of Medical Records in Patient Care, Compliance, and Hospital Operations
- Enhancing Patient Care – Accurate and readily available medical records support better diagnosis, treatment plans, and continuity of care. Quick access to a patient’s history reduces medical errors and improves clinical decision-making.
- Ensuring Compliance with Regulations – Healthcare facilities must adhere to strict legal and regulatory standards such as HIPAA (Health Insurance Portability and Accountability Act) and GDPR (General Data Protection Regulation) to protect patient privacy and confidentiality. Proper design of a medical records unit ensures compliance by incorporating security measures and restricted access protocols.
- Optimizing Hospital Operations – A well-organized records unit improves workflow efficiency, reducing retrieval time and administrative burdens. This contributes to better hospital management, cost reduction, and improved patient satisfaction.
If you want to know about the Types of slabs or Permeable concrete or Islamic architecture, please click the link.
1) Introduction
The function of the Medical Records Unit is the development and maintenance of health information systems involving the following:
- Retrieval, assembly, sorting and distribution of records for and to the wards and other patient units.
- Transcription / typing service for outpatient letters, discharge summaries and operation reports
- Classification (clinical coding) of diseases and procedures for inpatient admissions using an International Classification of Diseases
- Provision of information to management and other authorised staff for purposes such as planning, utilisation review, quality Assurance, casemix studies and research
- Quality assurance of the medical record to ensure standards are met.
The purpose of the Medical RecordsUnit is to provide for the secure maintenance, storage and retrieval of confidential clinical records. Provision should be made for 24 hour availability of clinical records either by a computerised or manual system.
A Health Facility must provide appropriate secure record storage and retrieval to ensure patient confidentiality at all times. A Health Facility must store all patient related administrative, historical and medical records in a fire rated construction as indicated in local bylaws.
2) Planning of Medical Records Unit
i) Operational Policies
Comprehensive examples of the issues on which unit decision-makers will be required to develop specific operational policies are listed below:
- A centralised record system should be maintained for all inpatient, emergency and outpatient/day patient attendances. Where a centralised system is not possible, the existence of a sub-file must be flagged to allow retrieval of the sub-file for patient care or medico-legal purposes.
- A unit numbering system will be used which will provide a single identifying number for every patient who presents to the Hospital i.e. the Medical Record Number (MRN). The MRN will be issued at the time of first admission or attendance and will be used for all subsequent admissions and treatment. Patient identification / registration must comply with Patient Registration standards.
- Accurate and up-to-date Patient Administration Systems will be maintained and information relating to patient movements will be updated as soon as the Department is notified.
- Terminal digit filing will be used in both active storage and secondary storage
- Correctly completed requests for each record leaving the unit will be required. The tracking of medical records will be facilitated by the use of bar coding on the record folder
- Information will only be released to a third party with the patient’s authority except if required for continuing patient care, or according to hospital operational policy.
- Medico-legal reports and subpoenas will be prepared in accordance with the Confidentiality Policy and relevant NSW Health Policy Directives.
- Medical records will be retrieved from secondary storage after hours only if deemed clinically necessary and staff may be accompanied by a security officer if necessary.
- A centralised dictating system utilising the telephone system may be used.
- Transcription of discharge summaries, operation reports and outpatient letters may be carried out in the Unit.
The record management system chosen will also require consideration of operational policies related to implementation of new technologies; cabling for departments; integration with existing communications systems; location of workstations; space and security requirements; air conditioning requirements and the transition process to be utilised when moving from one system to another.
Storage
Medical records must be kept for at least 10 or 15 years after last attendance or official contact or access by or on behalf of patient, or until the patient attains the age of 25 years, depending on Peer Hospital Group category.
If a commercial company is used to dispose of the records they should provide certification to confirm confidentiality. Records must be stored in a fire-rated construction as indicated in the local building bylaws. Note that sprinklers should NOT be installed.
Staffing levels
The Staff Establishment in a Unit based on hard copy files will include the following:
- Health Information Managers – a Unit Head of Department and additional professional staff depending on size of Unit
- Clinical coders
- Medical typists
- Administrative staff.
ii) Planning Models
Location
Location may depend on whether or not a pneumatic or mechanical automated records transport system is to be installed and the departments to which it is linked.
The decision to include such a system will strongly influence the external functional relationships of the Unit with the Outpatients Clinic area, in particular and may reduce the importance of direct access to the Emergency Unit.
It must be located so as to provide natural light and – if possible – views to staff who occupy the area during the working day. Planners must consider possible future uses of the unit envelope for such time as an electronic record system has evolved with consequent reduction in staff and diminishing storage needs.
The Unit should be considered as “soft” space into which an adjoining unit could expand or a new unit established. Secondary storage ideally will be readily accessible to minimise time wasted in access.
Building design
If a ground level location cannot be achieved, structural engineers must be consulted to calculate the weight of the records in order to ensure appropriate floor reinforcement.
iii) Functional Areas
Rooms, areas, or offices for the following personnel and/or functions shall be provided:
- Medical Records Administrator/ coding personnel
- Review and Dictation
- Sorting and Recording
- Microfilming of records, if applicable
- Record Storage, active and archived
Entry / Reception / Administration
A single controlled point of entry to the Medical RecordsUnit for the reception of visitors and staff. A temporary storage area will be required for returned files or files awaiting delivery to departments. A small amount of waiting will be required.
The optimum location for the offices for medico-legal staff is the Reception area with dual access from the Waiting Area and from inside the Unit.
Entry doors should have a buzzer and key card or similar for secure access for authorised staff. For units that run a 24 hour service, a peep hole in the door and/or a camera/intercom is required for after-hours access.
Access will be required within this area to Dictating / Research Cubicles so that visiting staff do not have to traverse the Unit.
Transcription
This area will provide the medical transcription service. Staff should be located in a quieter area of the unit but within close proximity to the dictating and general assembly/sorting area.
Consideration should be given to the acoustic treatment of this area as staff need to listen to transcription machines, however staff should not be totally separated from the other department activities.
Clinical coding
Coding requires an even greater degree of concentration to ensure accuracy so a quiet area is essential. Each coder will need a filing bay to store files awaiting attention plus storage for coding and reference manuals.
Offices
The staff side of the Reception Desk is a convenient location for offices for Health Information Managers to allow easy access for visitors to the Unit.
Photocopying / Printing
Dedicated, acoustically-treated and ventilated space is required. This space may also be used for generating bar code labels etc. This may also include stationery storage. Locate with ready access to the medico-legal offices that generate a large amount of photocopying.
Assembly & Sorting
An open plan area used for the processing activities associated with the filing and preparation of the medical records for clinics, admissions etc. including workstations and sorting tables. Each records officer will need a records storage bay and a trolley at or in close proximity to their workstation.
Storage will be required for:
- records awaiting sorting and assembly
- records awaiting filing
- newly assembled records
- Note that records awaiting medico-legal attention will be stored in the Medico-Legal Office As this area will be the major activity area of the Unit, it should have natural daylight. This area should be located with direct access to the filing storage areas and Photocopy & Stationery Store.
Shelving & Aisles
The most common and suitable method to file active medical records is on fixed metal shelving units (bays). Archived files may be stored in a compactus but a compactus is not recommended for active files as it can be dangerous and inconvenient if a number of staff wish to access files at the same time.
Standard bays are usually 900mm wide and 300mm deep. Regardless of the number of shelves in each bay (may be 7), the highest shelf should be accessible by a short member of staff using a library stool – usually six levels of shelving.
Step ladders are not recommended. Maximum height should be 2175mm. A minimum width of 750mm per aisle between facing bays must be provided; however for efficient retrieval of records, 900mm is recommended as it allows space for trolleys, library stools and for staff to pass each other in the aisles.
The main access aisle/s should be at least 1500mm wide to allow for trolleys passing each other, and for exit in the event of fire.
iv) Functional Relationships
In a traditional, “hard copy” environment, the critical relationship is with the Emergency Department for immediate record retrieval. Less critical is the relationship with Outpatients/ Ambulatory Care Units as files are usually pulled and delivered to the Units prior to clinic sessions. However, distances for transport of heavy records do need to be considered.
It is also useful to locate the Unit to encourage medical staff access to unwritten discharge summaries and for ease of access for record review etc. In a paperless environment, there will probably be no critical relationships except for staff wanting to access records still in hard copy for research purposes etc.
Archive file store
All the records requiring storage should meet the statutory requirements beyond the 5 year active storage period. There are a number of advantages for keeping non-active medical records readily accessible and available.
Two of these are:
- Time saving for staff;
- Easy access for refiling.
If storage space is a problem and microfilming or scanning of inactive records is being considered, a special room for microfilming will need to be planned.
The optimum solution is to locate the archival store within the Unit itself or directly underneath connected by a stairway. It is not often practical to include the space for all the records in a prime clinical area.
Consideration should be given to locating the records in a low activity area of the hospital and at the same time remain secure, dry and free from vermin, silverfish and other insects likely to attack the paper. Fire sprinklers should NOT be installed.
3) Design of Medical Records Unit
One main entry and exit for all staff and records is required to ensure the security and confidentiality of the unit and the medical record is maintained.
i) Environmental Considerations
Acoustics
Refer to () of these Guidelines.
Natural light
Essential in general work areas.
ii) Space Standards and Components
Ergonomics
Refer to () of these Guidelines.
iii) Safety and Security
Shelving and workbenches must meet Occupational Health & Safety Standards. Due to the confidential nature of the documents being handled in the Unit, careful consideration must be given to the security of the unit.
The unit should be secure at all times to protect the records against loss, damage or use by unauthorised personnel. There must also be adequate security for staff and visitors should not be able to enter the department proper without being let in by the receptionist.
The counter should be designed so that it would be difficult/ impossible to climb over. The required level of security can be achieved by limiting Unit entry / exit points to one (1) equipped with access control – keyed or electronic.
All other egress points should be locked and / or locally alarmed. Well signed, local alarms are a strong deterrent to unauthorised egress but the system must be overridden in the case of fire alarm activation in the area.
Hospital policy may require a security officer to accompany non medical records staff in the department where records are required after hours.
Optical Disc Security
Once a document is scanned, it cannot be lost or tampered with. By storing the original set of disks and using duplicates as working copies, complete sets of records are maintained at all times.
The second issue is security of access to the confidential records on the optical disk system. If a full system is implemented, terminals would be located throughout the Hospital.
This could pose problems for security of the information being accessed and displayed on these terminals. This means that safeguards must be put in place to prevent viewing of images by unauthorised persons.
System access and security systems must have multidimensional passwords that can avoid unauthorised intrusion into the system and particular records.
iv) Finishes
Wall Protection
Provide wall protection to all areas where trolleys are in use. Refer also to () of these Guidelines.
Ceiling and floor finishes
Refer also to () of these Guidelines.
v) Fixtures and Fittings
Refer to () of these Guidelines and to the Room Data Sheets (RDS) and Room Layout Sheets (RLS) for further detailed information
vi) Infection Control
Refer to () of these Guidelines for further information.
vii) Building Service Requirements
Information Technology / Communications
In addition to the usual hospital communication systems, the Medical RecordsUnit has particular needs. These include the need for remote dictating from the administrative and clinical areas to a central dictating unit.
Communication systems may include:
- office phones
- two-way intercom between designated staff areas or public address system in large units
- phone between the archival and main unit (if archives located off site or not adjacent to the main Medical Record Unit
- computer networking systems associated with the Medical Record technology
Duress alarm system
Locate duress alarms at Reception.
Lighting
Overhead lighting in the records store must run parallel to the direction of the filing bays to ensure adequate lighting of each aisle.
Floor Loading
Structural engineers must be consulted to calculate the weight of the records in order to ensure appropriate floor reinforcement if a ground level location cannot be provided.
4) Components of the Unit
The Medical RecordsUnit will contain a combination of Standard Components and Non-Standard Components. Provide Standard Components to comply with details in the Standard Components described in these Guidelines. Refer also to Standard Components Room Data Sheets and Room Layout Sheets.
i) Non Standard Components
Record Processing area
Description & Function – An open plan area used for the processing activities associated with the filing and preparation of medical records for clinics, admissions etc. It will incorporate parking for medical record transport trolleys. (Number and dimensions will need to be ascertained). This area may have “zones” for assembled files ready for issue and records waiting to be refiled. The area will need workstations and sorting tables.
Location & Functional relationships – This area should have direct access to the filing storage areas.
Considerations – At least part of this area should have access to natural light as it will be the major activity area of the department.
Dictation Cubicles
Description & function – The dictating area will be used by medical staff and others to view and research medical records as well as dictating and completing the discharge summaries.
Location & functional relationships – The cubicles should be located on the perimeter of the unit adjacent to but inside the reception area.
Considerations – The number of cubicles will depend on usage and the cubicles may be self contained or in an open plan office in which case cubicle partitions will be required. The auditory separation of personnel is preferred as extraneous noise will be distracting to the person dictating.
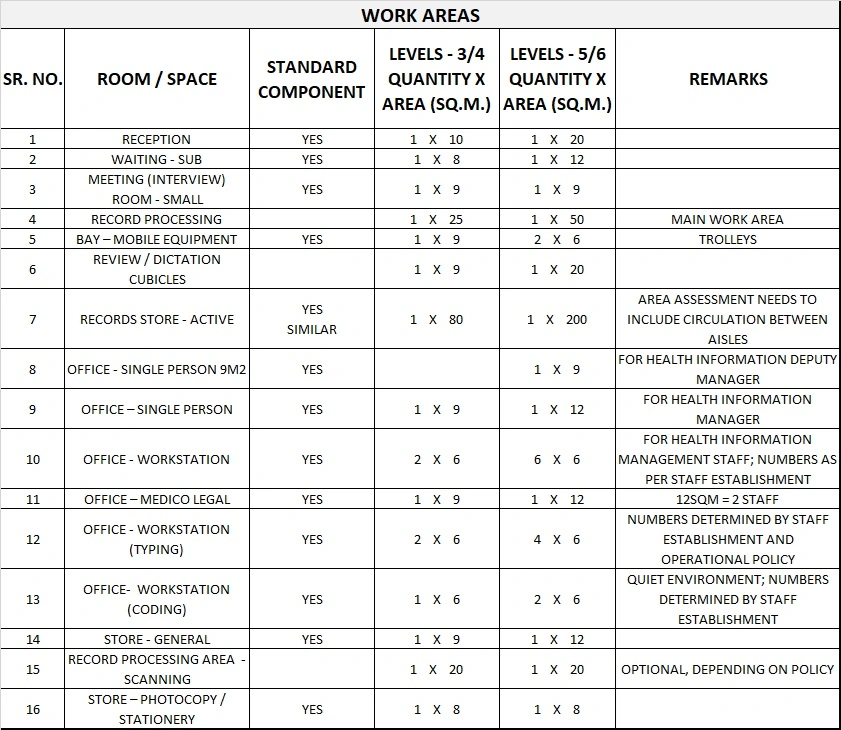
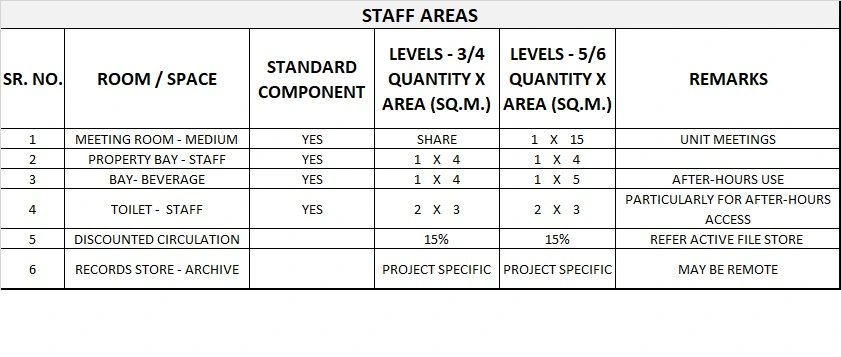
5) Schedule of Accommodation
Medical Records Unit Generic Schedule of Accommodation
Schedule of Accommodation for a Medical Records Unit at Levels 3/4 and 5/6 follows. Levels are assumed to provide the necessary support to the hospital overall.
Please note the following:
- Areas noted in Schedules of Accommodation take precedence over all other areas noted in the FPU.
- Rooms indicated in the schedule reflect the typical arrangement according to the Role Delineation.
- Exact requirements for room quantities and sizes will reflect Key Planning Units identified in the service plan and the policies of the Unit.
- Room sizes indicated should be viewed as a minimum requirement; variations are acceptable to reflect the needs of individual Unit.
- Office areas are to be provided according to the Unit role delineation and staffing establishment.
- Staff and support rooms may be shared between Functional Planning Units dependant on location and accessibility to each unit and may provide scope to reduce duplication of facilities.
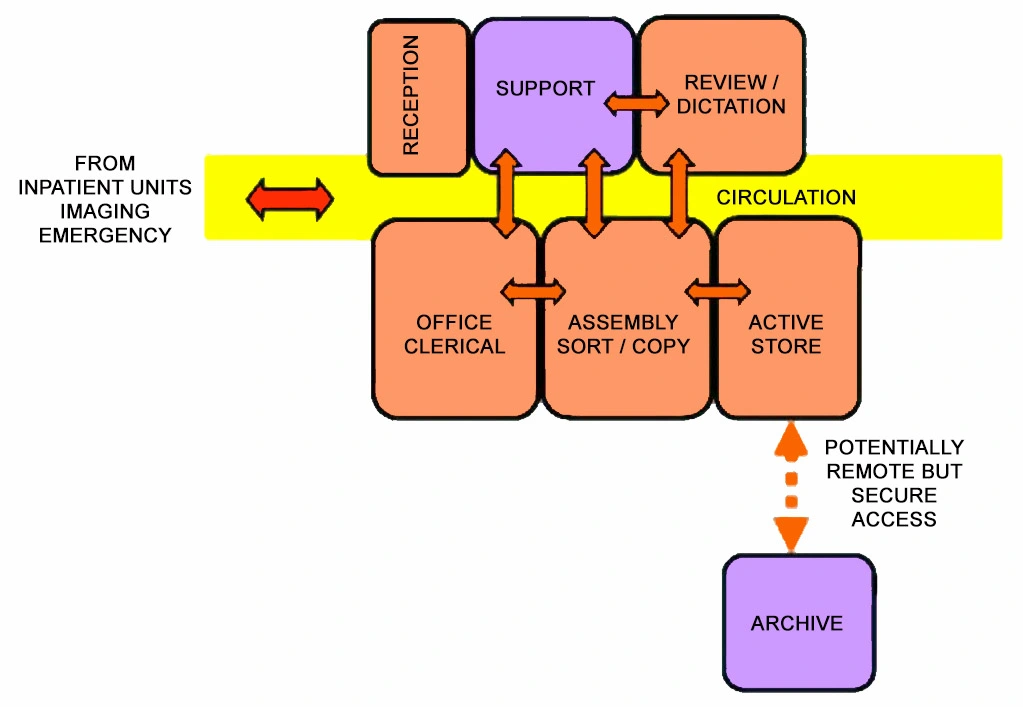
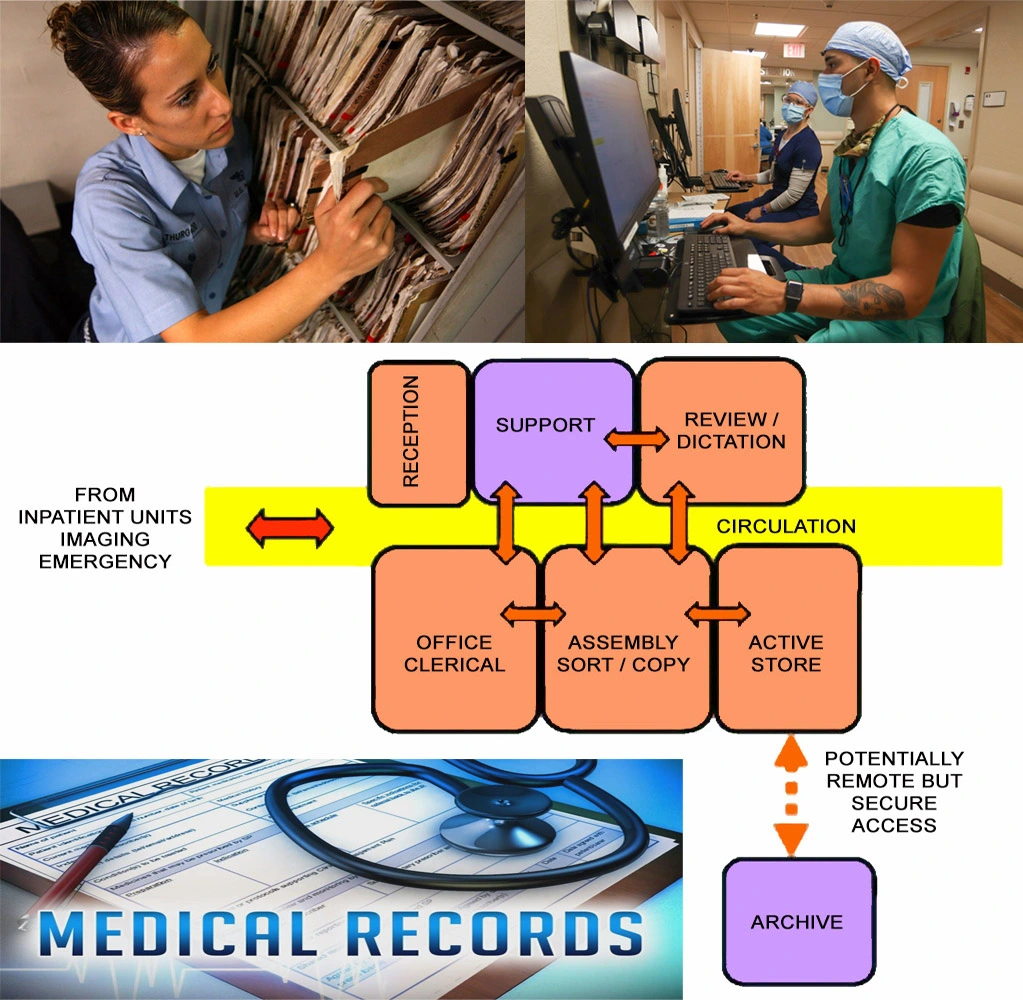
6) Functional Relationship Diagram
Medical Records Unit Functional Relationship Diagram